Indice del volumen
Volume index
Comité Editorial
Editorial Board
Comité Científico
Scientific Committee
NEUROEPIDEMIOLOGICAL SURVEY FOR EPILEPSY AND KNOWLEDGE ABOUT NEUROCYSTICIERCOSIS AT SIDWADWENI LOCATION, SOUTH AFRICA.
Foyaca-Sibat H, Del Rio AR, Ibanez-Valdes LdeF, Vega-Novoa E del C, Awotedu AA.
University of Transkei. Faculty of Health Sciences. Department of Neurology, Department of Community Medicine, Department of Family Medicine.Division of Medicine. Private Bag X1, Umtata 5900 South Africa
Rev Electron Biomed / Electron J Biomed 2004;1:40-48.
Commentary of Prof. Marco Tulio Medina. Director Postgrado de Neurologia. Universidad Nacional Autonoma de Honduras. Tegucigalpa, Honduras.
Commentary of Prof. Sanjib Kumar Sharma MD. Department of Medicine, BP Koirala Institute of Health Sciences, Dharan, Nepal.
Key words: Epidemiology, neurocysticercosis, and epilepsy.
ABSTRACT:
Objective To determine the prevalence of epilepsy and to screening knowledge about neurocysiticercosis (NCC) and HIV/AIDS in adult population of one South Africa rural community.
Setting: Sidwadweni community, at 30 km away from Umtata (Capital of the former Transkei).
Design: A two-stage design study was used. The first stage involved screening of the general population on door-to-door basis by interviewing peoples living in 100 household selected by block-randomisation procedure using an internationally validated questionnaire for detecting epilepsy and knowledge about some associated diseases. The second stage consisted of a neurological assessment of the peoples who screened positive.
Results: A total of adults were screened. The prevalence of active epilepsy among adult population was 3.6/1000, and 4.7/1000 in children. Most of epileptic patients were not under regular anti-epileptic treatment, 87 % of the total population had not idea about NCC, but only 10 % did not know the cause of AIDS.
Conclusions: The prevalence of epilepsy is not very high compared with a similar community but a poor utilization of anti-epileptic treatment is cause for concern. Traditional belief’s roots on this community are considerably deep. HIV/AIDS awareness campaign for Sidwadweni is functional, and a similar campaign for prevention of NCC should be performed while permanent solutions are implemented.
INTRODUCTION
Prevalence of Epilepsy has not been established at the former Transkei before this study.
Neurocisticercosis (NCC) is an infection of central nervous system (CNS) caused by the larval stage (Cysticercus cellulosae) of the pig tapeworm Taenia solium. This is the most common helminthes to produce CNS infection in human being. The occurrence of acquired epilepsy or the syndrome of raised intracranial pressure in a person living in or visiting a region where taeniasis is endemic or even in one living in close contact with people who have taeniasis should suggest a diagnosis of cysticercosis; patients with NCC may remain asymptomatic for months to years, and commonly a diagnosis is made incidentally when neuroimaging is performed, many symptomatic forms can predominate. Symptoms and signs are related both to the parasite, which can show a different biological behavior from one place to another, and different inflammatory-inmunological responses on different hosts.
NCC is the most common cause of acquired epilepsy worldwide and most of the patients taking phenytoin or carbamazepine for a proper control of their seizures, respond very well. 1 2 3 4 5 Other aspects related to NCC from our region are also available on line 6 7 this study was designed for Sdwadweni location which is situated at the former Transkei. This region was one of the three administrative authorities of the so-called independent homelands (Ciskei, Transkei and the Cape Provincial Administration under different apartheid governments) it is currently region D and E of Eastern Cape Province of South Africa; Umtata is the capital for the former Transkei which is one of the poorest region countrywide, and serves as a labor reservoir for other wealthier provinces, with men leaving behind women and children whilst they seek and find employment elsewhere.8
The main objective of this study is to determine the prevalence of epilepsy, and the knowledge about NCC and HIV/AIDS as conditions extremely frequent associated with recurrent epileptic seizures and other epidemiological aspect from one of our rural locations at Qumbu municipality situated 30 Km away from Umtata.
MATERIAL AND METHOD:
Sdwadweni is one of the largest communities situated across the N2 highway near to Umtata west. Mhlakulo health centre located at the same area serves it. The Mhlakulo health offers primary health care services to other rural communities from this municipality, and two family doctors and 6 registered nurses staffed it at the prevalence day. The portion of Sidwadweni that was surveyed was on the N2 highway, across the road from Mhlakulo Health Centre.
A team of 12 senior medical students from University of Transkei (Unitra) in South Africa trained in the diagnosis of epilepsy and NCC implemented the questionnaire, the survey was made according to a World Health Organization protocol (1981). The training consisted of a series of seminars, graphic bibliographic material and PBL (Problem Based Learning) tutorials about these topics. They administered a standard screening instrument for epilepsy, NCC, HIV/AIDS, and socioeconomic living conditions among other issues. After to be introduced to the CHESP coordinator for the community, the group was divided into smaller group of two member each, where at least one was fluent in Xhosa (the native language). The survey was conducted between 12 and 16 hrs when most of the men would be out working therefore most of interviewed were women
The study was outlined in two stages, and the investigation was door-to-door in a total of 100 houses selected by block-randomization procedure. Since its foundation Sidadwedweni community was interviewed for the time along this study. First phase consisted in preparation, co-ordination through community’s leaders, training and data collection, and the second one for reassessment of identified candidates and processing of findings.
RESULTS
The results of the instrument showed a sensitivity of 86% (CI-94%, 83.7-95), specificity of 96% (CI-94,85-97). On screening, the positive subjects found re-assessed by one of us being also a number of inhabitants women twice fold than men.
On the basis of the definition proposed by the International League Against Epilepsy, we detected a prevalence of 3.6/1 000 (Table I) among adults and 4.7/1000 in children. Fifty six percent of the total group had active epilepsy on the prevalence day (October 14th, 2003).
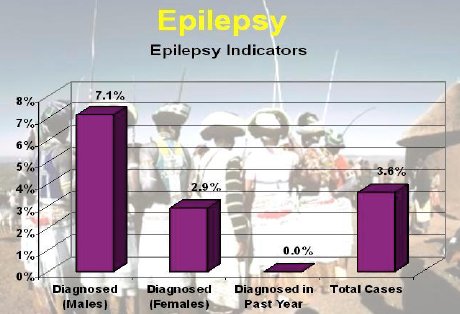
Table I: Low prevalence of epilepsy compared with similar location
(Ngqwala 13.7/1 000) at the same prevalence day.
The mean age of age at onset was 23.7 years for motor partial epileptic seizures and 12,3 years for generalized seizures. More than 50% of the total population had some knowledge about epilepsy (Table II), but most of them interpreted epilepsy associated with some evil spirits (Table III).
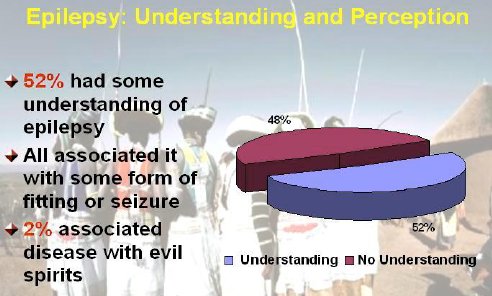
Table II: Most of the interviewed had some knowledge about epilepsy.
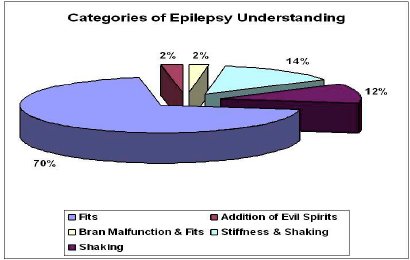
Table III: Few respondents considered epilepsy due to evil spirits but
most of peoples indicated that there was an associated spiritual component.
Only 33 % of patients had received anti-epileptic medication for more than three month (Table IV) and only 5 % of them received medication for six consecutives months.
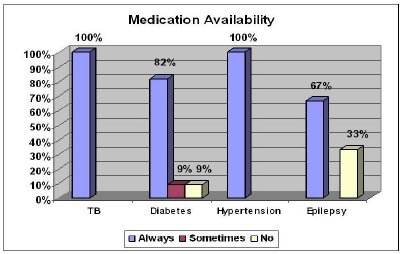
Table IV: Medication for epilepsy often goes out of stock because they are
Special Order Drugs (ordered every two weeks), and the Mhlakulo
Health Centre does not have adequate transport facilities.
In spite of the high qualifications of the interviewers whom had not communication problems due to language-barrier a number epileptic patients were probably not reported because of poor recognition of some non-convulsive epileptic attacks, traditional beliefs, cultural traditions, and stigmas associated with epilepsy.
Socioeconomic status in general was characterized by unemployment or very low salaries, limited access to primary health care and health education, limited access to toilet facilities, proper refusal disposal, safe and clean water, lack of education of the most peoples to limit access of pigs to human feces while free-range pig farming is commonly practiced. Most of the population (87%) did not know about NCC (Table V). Pork meat consumption is high at least once a month (Table VI) and the preferred method for coking was boiling (Table VII).
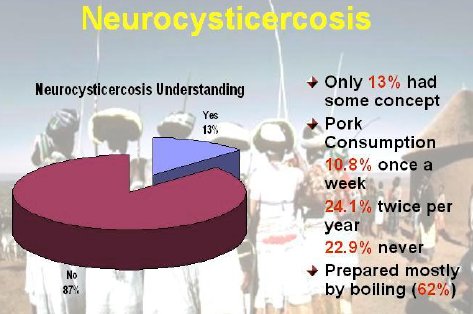
Table V: Most of the population have no idea about neurocysticercosis.
13% of the respondents were able to say that it was an infection associated with pork and it affect the brain.
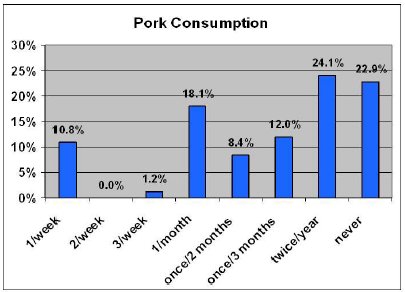
Table VI: Just over a tenth of the sample eats pork on a regular basis.
At Ngqwala only 1.5 % of the surveyed eat pork meat once a week.
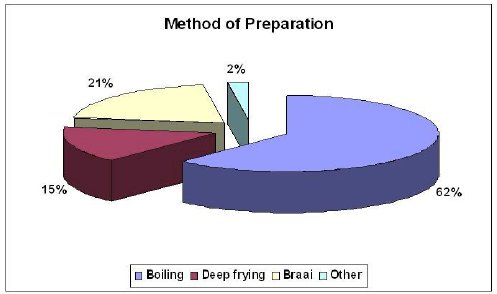
Table VII: For cultural and economic reasons, boiling seems to be
the preferred method of pork meat preparation.
DISCUSSION
The philosophy of University of Transkei is based on Problem Based Learning (PBL) curriculum therefore our students are enabled to conduct their own community diagnosis. This has been achieved due to the implementation of the COBES (Community Based Education System) programmed, which provides an opportunity for medical students to observe and experience the communities they may serve in future.
Epilepsy is the most common chronic disorder of the central nervous system (CNS) manifested by recurrent unprovoked seizures that affect approximately 1% of the U.S. population,9 in our province the amount of people affected remain unknown for reasons that will discuss below. During 1986-1990 approximately 1.1 million persons in United States annually reported having epilepsy and the overall prevalence of epilepsy was 4.7. The point prevalence of epilepsy is estimated at about 0.4 % to 0.8 % in some European countries,10 11 the prevalence of epilepsy is said to be about 3 to 9 per 1,000 population. As countries in Asia, the prevalence rates from published reports are: China (4.6),12 Parsi (4.7), Kashmir (2.47) rural Bengal also in India (3.05)13 Pakistan (9.0), Guam (4.9), Singapore (3.5), rural Thailand (7.2)14 and the Philippines League Against Epilepsy (2.3). The lower prevalence rate reported in the last study was most likely related to differences in the communities surveyed, because the Philippine study was conducted in a mixed urban and rural community.15 Central and South American countries exhibit high prevalence rate of epilepsy compare with North America. In Andean region of Ecuador lifetime point-prevalence rates between 12.2/1000 and 19.5/1000 were recorded16 rural Bolivia (12.3) confirming that epilepsy is a major health problem in rural areas of developing countries17 African countries show different prevalence rates from Gambia (4.6),18 to Benin (15.9).19 However, that prevalence in Gambia may be an underestimate as some studies from other developing countries (such as Colombia, Liberia, Togo, Bangladesh, Cameroon, Mali, Madagascar, West Uganda, Nigeria, Panama, United Republic of Tanzania and Venezuela) suggest a prevalence of more than 10 per 1,000. In 2000 a two-phase design study for to determine the prevalence of epilepsy in rural South Africa children aged 2-9 years was done showing a prevalence rate of 7.3/1 000.20 A similar study was performed by us at Ngqwala location for adult population showed a prevalence of 13.7/1 000.21Taking in consideration that Sidwadweni has similar socio-economic characteristic, and considering also that this study was done at the period of time obviously other reasons should explain that remarkable difference. We though that cultural and traditional belief strongly contributed to report a considerable less amount of peoples suffering epilepsy. It’s almost sure that an exact prevalence of epilepsy on that area will be detected in many years.
Because South Africa is a diverse country that represents peoples of different cultural background, who also are living in environment completely different for each others, the former Transkei does not escape to that sentence which is also enriched by the consequences of poverty and underdevelopment compare with other more advantage areas of this country. Throughout these different regions, exist various traditional beliefs pertaining to epilepsy and its causes and treatment. NCC is the most common cause of acquired epilepsy in Transkei3 being a preventable disease with a tendency to increase and spread all over the country gradually if not effective measure are taken.
Our survey found that only 7.6 % of epileptic patients were under regular anti-epileptic treatment for the past three consecutive months. Most of epileptic patients are under traditional treatment taking herbal remedies with "anti-seizure effect," and some of them die due to herbal intoxication leading to acute renal failure when wrong mixtures of plants, wrong selection or preparation, and/or incorrect storage are made. Speaking-Xhosa sangomas treat an important number of epileptic patients because epilepsy is thought to be related to a visitation by the devil, to witchcraft or to spirits, and those families also belief that they have been visited by their ancestors, whom arriving at night while they are sleeping; they also consider that the first place for visiting is the toilet being it another powerful reason why they do not use the toilet more often in spite of its availability.
In other places epilepsy is thought is a disease where the heart gets blocked by foam, restricting circulation and resulting in seizure. One generalized belief is that Xhosa-sangomas shaking some bones and helped by their ancestors can find out the cause of the problem and treat it. Conventional medical care was not available for peoples living in most of those region during apartheid era therefore almost all traditional medicines and cures were made from available material, such as leaves, roots, spider webs, axle grease, and water among other products.
We have many species of plants in flower throughout the year but the greatest displays are over the short spring during the period from late August to early October. It is an area of moderate winter and hot dry summers when temperature can reach 38o C. The average annual rainfall over the area varies between 125 and 350 mm, virtually all of it falling between April and September. Most of our medical plants grow up on sandy costal flats or sandy soils among rocks, often granite, costal bush or deep forest with very difficult access reason being it another explanation for unavailability of herbal medication, misreplacement or miscombination leading to intoxication; nevertheless if the patient does not develop complications then an acceptable outcome may be observed because placebo effect play a large role in traditional medication on strong religious and spiritual belief of the patient.
Many studies have shown that there are still many misconceptions existing within many cultural communities, where only tonic-clonic seizures are recognized as epilepsy and non-epileptic seizures are labelled as nervous disturbances, emotional stress or insanity, and for most of peoples member of those community epilepsy is still considered an infectious disease an invasion by supernatural unknown spirit or ancestors. Poverty, poor food hygiene and sanitation, lower cultural level, myths and superstitions attached with epilepsy on those region impede to move forward in the early detection of the disease, identification of their causes, and an adequate management.
As before-mentioned, that misinformation about epilepsy (among other explanations) will impede to establish the exact number of untreated epileptic patients, and it will remind unknown for a long time until a sustained campaign to build up public awareness on this matter, and a better health education plus alleviation of poverty among other factors will take effect. Same statement should be applied to NCC awareness campaign in order to reduce the increasing number of epileptic patients due to NCC.
ACKNOWLEDGEMENTS: We are very grateful to the medical students: A. S. Ganesan, A. U. Mxoli, V. P. Ndabeni, M. E. Nombembe, R. D. Sapinoso, M. P. Sompetha, R. A. Wilson, V. Yokwe, V. J. Gela, L. Jordan, K. Maharaj, P. Mkabile, D. T. Mda, and P. Mkondweni.
REFERENCES.
1. - Foyaca SH, Iba&ñez V.LdeF, Awotedu A, Fernandez MC. Neurocysticercosis in critical stage. Third International Congress of critical care medicine on Internet. 2. - Foyaca SH, Iba&ñez V.LdeF. Clinical trial of praziquantel and prednisone in rural patients with neurocysticercosis presenting recurrent epileptic attacks. The Internet Journal of Neurology 2002;1(2):34-51. 3. - Foyaca SH, Iba&ñez V. LdeF, Awotedu A, Fernandez MC. Neurocysticercosis in the former Transkei. 7th Internet World Congress for Biomedical Sciences INABIS 2002. 4. - Foyaca SH. Tapeworm and the brain. Science in Africa. June 2002;XVIII:3. 5- Foyaca SH, Iba&ñez V.LdeF. Intraventricular neurocysticercosis. II Virtual Congress of Neurosurgery. 6- Foyaca S.H, Ibanez V. LdeF. Vascular dementia type Binswanger’s disease in patients with active neurocysticercosis. Elect J Biomed 2002;1(1):1-12 7- Foyaca S.H, Ibanez V.LdeF. Enfermedad de Binswanger en pacientes con neurocisticercosis activa. IV Internet Congreso de Psiquiatria Interpsiquis2003. 8- Mahlalela X, Rohde J, Meidany F, Hitchinson P, Bennett J. Primay Health Care in the Eastern Cape province. 1997-2000 EQUITY PROYECT. South Africa Department of Health.
9. - Hauser WA, Headorferr DC. Epilepsy: frequency, causes and consequences. New York: Epilepsy Foundation of America, 1990.
10. - Hauser WA. Incidence and Prevalence, Epilepsy: A comprehensive Textbook, Engel J, Pedley TA and Jr (eds): Lippincott-Raven, 1997:47-57.
11. - Forsgren L. Prevalence of Epilepsy in Adults in Northern Sweden. Epilepsia 1992;33(3):450-458.
12.-Epilepsy Foundation. Status and developing. 13. - Das Sk, Sanyal K. Neuroepidemiology of major neurological disorder in rural Bengal. Neurol India 1996;44(2):47-58.
14. -Asawavichienjinda T, Sitthi-Amoru C, Tanyanont W. Prevalence of epilepsy in rural Thailand: a population-based study. J Med Assoc Thai 2002;85(10):73.
15.-Epilepsy. General information. Available online at: http://www.plae.org/web/epilepsy-information4.php
16. - Placencia M, Shorvon SD, Paredes V, Bimos C, Sander JW, Suarez J, Cascante SM. Epileptic seizures in an Adean region of Ecuador. Incidence and prevalence and regional variation. Brain 1992;115(30:771-782.
17. - Nicoletti A, Regio A, Bartoloni A, Failla G et al Prevalence of epilepsy in rural Bolivia; a door-to-door survey. Neurology 1999;53(9):2064-2069.
18. - Bulletin of the World Health Organization 2002;80(5):378-383.
19. - Debrock C, Preux P-M, Houinato D, Druet-Cabnac M, Kassa F et al Estimation of prevalence of epilepsy in the Benin region of Zinvie using the capture-recapture method. Int J Epidemiol 2000;29:330-335.
20. - Chritianson AL, Zwane ME, Manga P, Rosen E, Venter A, Kromberg JG. Epilepsy in rural South African children-prevalence, associated disability and management. S Afr Med J.2000;90(3):262-266.
21. - Foyaca-Sibat H, Del Rio A R, Ibanez-Valdes LdeF, Vega E. Neuro-epidemilogicalsurvey for epilepsy and knowledge about neurocysticercosis at Ngqwala location, South Africa. The Internet Journal of Neurology. 2004;1(1):21-34 Also available online at: http://www.ispub.com
http://www.uninet.edu/cimc2001/comunicaciones/foyaca/index.html
Available from: http://www.ispub.com
http://www.inabis2002.org/poster_congress/area_01/01011/010117.pdf
http://www.scienceinafrica.co.za/2002/june/worm.htm
http://www.neuroc.sld.cu/papers/tl-neurocys.htm
Available online at: http://www.uninet.edu/biomed/rebio/reb/2002/n1/foyaca.html
Available online at: http://www.psiquiatria.com/interpsiquis2003/9638
Available online at:http://www.epilepsyfoundation.org/epilepsyusa/developing.cfm
Commentary of Prof. Marco Tulio Medina. Director Postgrado de Neurologia. Universidad Nacional Autonoma de Honduras. Tegucigalpa, Honduras.
Es este un articulo excelente y de mucha relevancia epidemiologica. Efectivamente una de las principales causas prevenibles de epilepsia en los paises en vias de desarrollo es la neurocisticercosis, de tal manera que la evaluacion comunitaria del conocimiento de esta parasitosis es importante para la planificacion ulterior de estrategias educativas que reduzcan tanto la neucisticercosis como la epilepsia.
Commentary of Prof. Sanjib Kumar Sharma MD. Department of Medicine, BP Koirala Institute of Health Sciences, Dharan, Nepal.
The interest of this paper is that it provides baseline data on prevalence of Epilepsy and knowledge about Neurocysticiercosis and HIV/AIDS in the adult population of rural community of South Africa.
Received: January 11, 2004.
Published: February 19, 2004