Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
SYNDROME OF INADEQUATE SECRETION OF ANTIDIURETIC HORMONE ASSOCIATED TO PULMONARY THROMBOEMBOLISM:
A NON-DESCRIBED CAUSE OF HYPONATREMIA
IN THE LITERATURE.
Carlos G. Musso1-2, Vilas M1-2, Chiapella M2, Conti P2, Reynaldi J1,
Mombelli C1, Navarro M1, Frydelund S1, Algranati L1.
1Servicio de Nefrología. Hospital Italiano de Buenos Aires. 2Centro Médico Agustin Rocca
Buenos Aires. Argentina
carlos.musso @ hospitalitaliano.org.ar
Rev Electron Biomed / Electron J Biomed 2008;2:59-61
SUMMARY
Syndrome of inadequate secretion of antidiuretic hormone (SIADH) is a condition that can be associated to various sort of lung diseases.
In this report we present a clinical case where a SIADH associated to pulmonary thromboembolism was documented. As long as we know, this association has not been described yet in the literature, and we hypothesized that lung cytokines released due to pulmonary necrosis could be the main stimulus to vasopressin secretion in this entity.
Conclusion: Pulmonary thromboembolism should be incorporated in the list of lung causes of SIADH.
KEY WORDS: Syndrome of Inadequate Secretion of Antidiuretic Hormone (SIADH). Pulmonary Thromboembolism
RESUMEN
El síndrome de secreción inadecuada de hormona antidiurética (SIADH) es una condición que puede asociarse a diversas neumopatías.
En el presente reporte clínico se presenta un caso de SIHAD asociado a un tromboembolismo pulmonar. Hasta donde sabemos, la asociación entre TEP y SIHAD no había sido reportada aun en la literatura, y presentamos como hipótesis etiológica la liberación de citoquinas inductoras de la secreción de vasopresina, secundaria al daño parenquimatoso pulmonar del TEP.
Conclusion: El tromboembolismo de pulmón podría ser incorporado a las causas pulmonares de SIADH.
PALABRAS CLAVE: Síndrome de Secreción Inadecuada de Hormona Antidiurética. Tromboembolismo Pulmonar
INTRODUCTION
Syndrome of inadequate secretion of antidiuretic hormone (SIADH) is a condition which typically presents hipo-osmolar hyponatremia with normal extracellular liquid and high fractional excretion of urea (> 55%) in the absence of hypothyroidism, cortisol deficit, renal failure, and hyponatremia inducing drugs 1.
Among the causes of SIADH we find those related to various sort of lung diseases, nevertheless no report to date has included hyponatremia associated to pulmonary thromboembolism (PTE) as one of them2. Thus, we present the following report where such association was documented
CASE REPORT:
72 year-old-female patient with a history of hypertension treated and normalized with low sodium diet (she had no need neither of diuretics nor other antihypertensive drugs); and multiple myeloma treated with thalidomide. She was hospitalized suffering from a sudden episode of dyspnea and pulmonary infiltration on the X-ray which was interpreted as secondary to PTE. Then this suspicion was corroborated by a pulmonary CT angio scan.
Together with the PTE diagnosis, it was also documented an acute hypo-osmolar hyponatremia in the absence of illnesses or drugs which could potentially cause such dysnatremia. Besides, she had no thoracic pain nor fever and it was not documented neither hypothyroidism, cardiac failure, nor cortisol deficiency in her analysis. Her serum glucose level and blood pressure were in normal range.
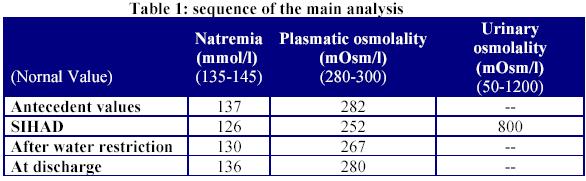
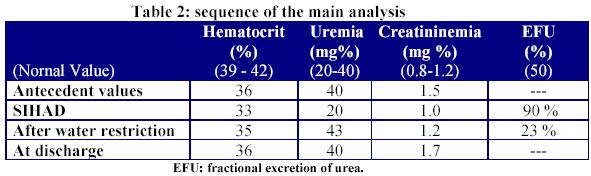
The patient was treated with anticoagulation (heparin) and water restriction as measures for her PTE and SIAHD respectively. After initiating that treatment, the patient´s natremia was normalized and she was discharged from the hospital (Tables 1 and 2).
DISCUSSION:
It has already been reported some causes of SIAHD secondary to pulmonary diseases. In these settings, the mechanism proposed as the cause of this phenomenon would be the release of hyponatremia inducing cytokines by the damaged lung parenchyma. Among pulmonary diseases that were described as potential cause of SIHAD it can be found: pneumonia (viral, bacterial, tuberculosis, micotic), lung abscess, asthma, atelectasis, pneumo-thorax and fibrocystic diseases. Regarding pulmonary tumors, such as the small cell carcinoma, they could induce SIHAD by a paraneoplastic mechanism, which consist of an ectopic vasopressin secretion 1-3.
Pain can be another cause of vasopressin release4 but it was not present in this case report where the only PTE symptom was the sudden appearance of dyspnea.
Concerning the present described hypotranemia (associated to pulmonary thromboembolism), it could be caused by vasopressin secretion inducing cytokines released due to lung necrosis.
CONCLUSION:
Pulmonary thromboembolism could be considered another cause of SIADH secondary to lung damage.
REFERENCES
- 1.- Ellison D, Berl T. The síndrome of inappropriate antidiuresis. NEJM. 2007; 356: 2064-2072
2.- Martinez-Maldonado M. Inappropriate antidiuretic hormone secretion of unknown origin. Kidney Int. 1980; 17: 554-567
3.- Clinicopathologic Conference. Fever, respiratory tract symptoms and hyponatremia. The American Journal of Medicine. 1980; 69: 309-320
4.- Robertson G, Berl T. Pathophysiology of water metabolism. In Brenner B (ed). The kidney. Philadelphia. W.B. Saunders. 1996: 873-928
Received: April 28, 2008. Received reviewed June 17, 2008
Published July 12, 2008.