Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
Letters to the Editor / Cartas al Editor
SUBCUTANEOUS EMPHYSEMA A COMPLICATION
OF CRYOTHERAPY
L. Sempau, C. Hidalgo, MC Gutierrez
Department of Dermatology. Hospital Universitario de Burgos. Spain
Rev Electron Biomed / Electron J Biomed 2014;3:61-63.
To the Editor:
We present an 86 year-old patient, with a history of chronic bronchitis, hypercholesterolemia, hypertension, and thrombocytopenia treated with bronchodilators, inhaled corticosteroids, antihypertensive and antiplatelet drugs, who consulted for erythematous lesions, with some type of cutaneous horns on the face, back of hands and forearms, consistent with actinic keratoses.
It was decided to perform curettage before cryotherapy on the hyperkeratotic lesions.
On applying cryotherapy to a lesion on the right temple, there was sudden swelling and whitening of the temple, as well as the ipsilateral eyelid. Fig.1.
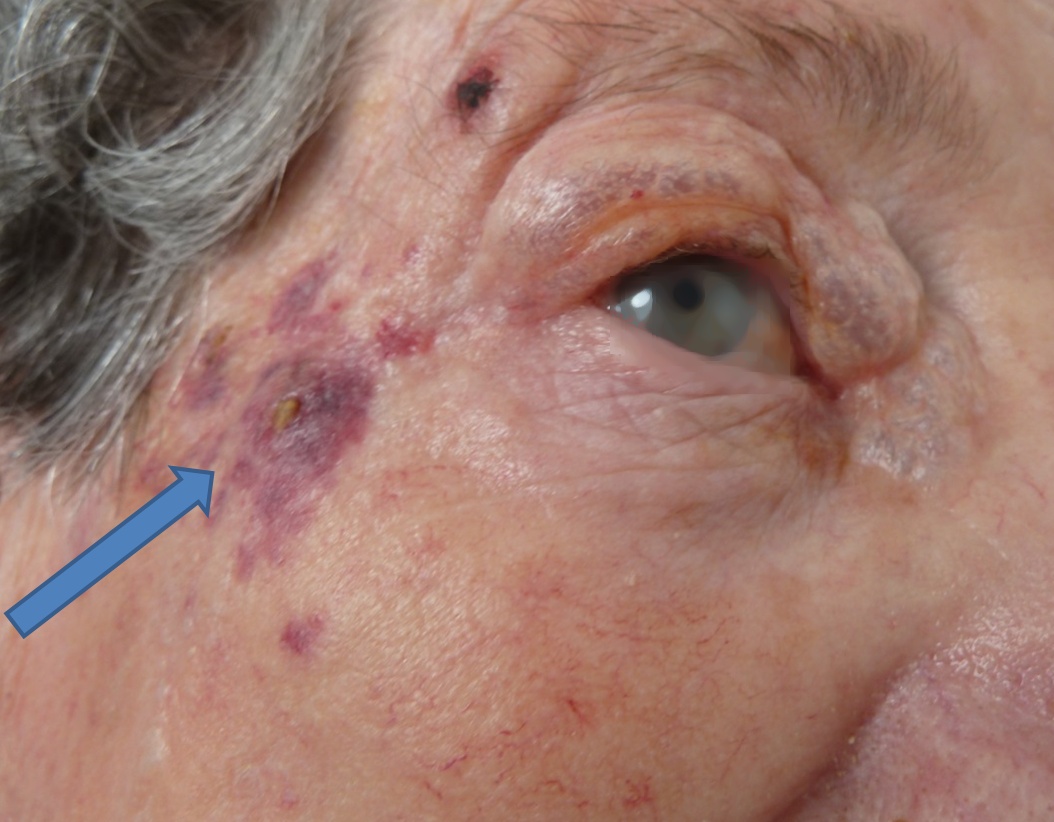
Figure 1: Arrow at the site of application of cryotherapy and swelling of the eyelid.
The white color disappeared after a few seconds, leaving the eyelid swollen, with crepitus on palpation.
The patient only complained of pain at the point of application of cryotherapy and of some difficulty in opening eyelids, which resolved within minutes, on redistributing the air by the eyelid and inner canthus. Fig.2.

Figure 2: Eyelid swollen with crepitus on palpation.
The subcutaneous emphysema was resorbed spontaneously without sequelae after a week. Fig.3.
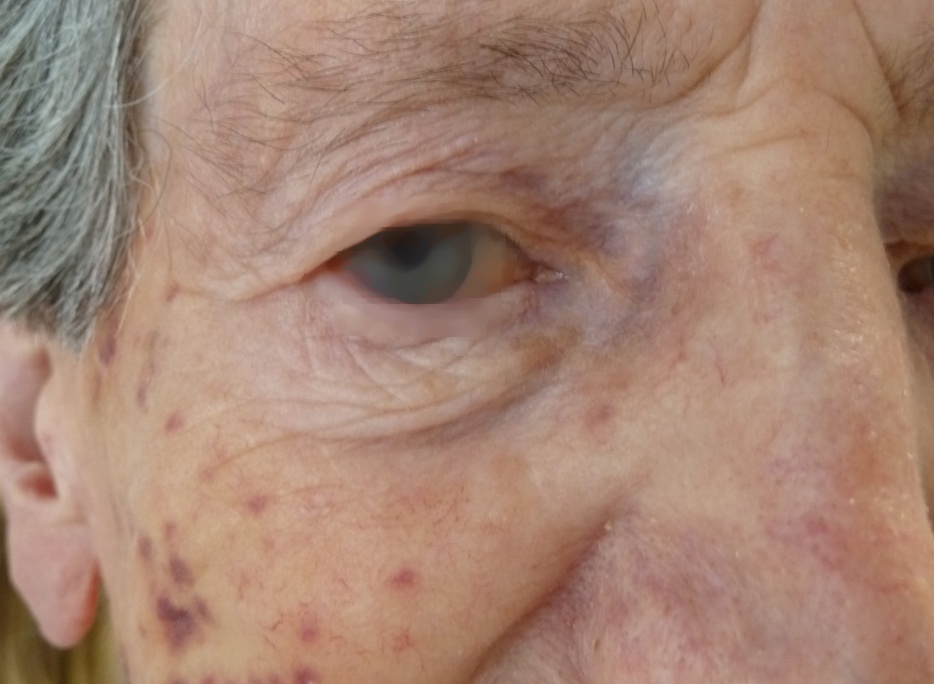
Figure 3: Appearance of the patient's face several days later
Several adverse effects of cryotherapy spray have been reported, some immediate such as pain, swelling and blistering, and others permanent, with hypo- and hyperpigmentation, necrosis and changes in deeper structures such as the nail matrix, peripheral nerves, or hair follicles1-2.
There are very few cases in the literature of subcutaneous emphysema secondary to spray cryotherapy applied externally to treat skin lesions3-5. There are another two cases of subcutaneous emphysema described in literature: one in the treatment of femoral chondroid tumor, which had noted a leak in the cryoprobe6 and the other in an endoscopic cryoablation for Barrett's esophagus7.
In our case, the prior curettage of cutaneous horn in photodamaged skin, conditioned the rapid dissection of tissues by the gas pressure to reach the eyelid.
CONCLUSIONS
The application of cryotherapy spray on epidermal continuity solutions can cause tissue dissection in patients with atrophic dermis and solar elastosis usually common in patients with actinic keratosis.
It should be also noted that the continued use of inhaled corticosteroids causes skin atrophy that is often underestimated by physicians.
REFERENCES
1.- Thai KE, Fergin P, Freeman M, Vinciullo C, Francis D, Spelman et al. A prospective study of the use of cryosurgery for the treatment of actinic keratoses. Int J Dermatol 2004;4:687-92
2.- Zouboulis CC: Cryosurgery in Dermatology. Eur J Dermatology 1998;8:466-7
3.- Jensen P, Johansen UB , Thyssen JP: Cryotherapy caused widespread subcutaneous emphysema mimicking angiooedema. Derm Venereol 2014; 94: 241,
4.- Vano-Galvan S, Bagazgoitia L, Perez B, Jaen P. Subcutaneous emphysema caused by cryotherapy application over a corticosteroid-induced atrophic skin. J Eur Acad Dermatol Venereol 2008;22(4):508-9.
5.- Lambert TJ, Wells MJ, Wisniewski KW. Subcutaneous emphysema resulting from liquid nitrogen spray. J Am Acad Dermatol 2006;55(5 Suppl):S95-6.
6.- Kadic, L, Driessen JJ. Sybcutaneous emphysema after cryosrugery of a lesion of the femur during femoral nerve block. J Clin Anesth 2011;23:255-7
7.- Chaudhry T, Hafez O, Barthel JS. Transient facial subcutaneous emphysema: an unusual complication of liquid nitrogen spray cryoablation of Barrett's esophagus. Gastrointest Endosc 2012;75:1283-5
CORRESPONDENCE:
Dra. Leticia Sempau.
Servicio de Dermatología.
Hospital Universitario de Burgos.
Avda. Islas Baleares 3,
09006 Burgos
Spain
Mail: leticiasempau @ gmail.com