Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
- low body urea production, as is the case of malnutrition, hepatic insufficiency, etc
- increased excretion of urea, as is the case of proximal tubular dysfunction (Fanconi syndrome), osmotic diuresis (glucosuria, etc), water diuresis (diabetes insipidus), urea tubular secretion (syndrome of inappropriate antidiuretic hormone secretion), etc6
- a non-oliguric acute renal failure secondary to a pyelonephritic process. This situation could be justified since this infection took place in an aged single kidney patient.
- a nephrogenic diabetes insipidus (water diuresis) secondary to the renal interstitium alteration induced by the acute pyelonephritis.
- an elevated urea excretion secondary to a reduced water reabsorption capability and intra-renal urea reciclying process. Both disorders could be induced by the acute pyelonephritis. This increase in the fractional excretion of urea could explain the normal plasma urea levels found in our patient despite of his reduced glomerular filtration.
ACUTE RENAL FAILURE WITH NORMAL PLASMA UREA LEVEL
SECONDARY TO ACUTE PYELONEPHITIS IN A SINGLE KIDNEY PATIENT
Musso CG1, 2, Vilas M1, 2, Fernandez Otero L2, Imperiali N1, Algranati L1
1Nephrology Department. Hospital Italiano de Buenos Aires.
Centro Medico Agustin Rocca2. Argentina
carlos.musso @ hospitalitaliano.org.ar
Rev Electron Biomed / Electron J Biomed 2007;1:42-44
Versión en español
Comment of the reviewer Jeyaraj Balasubramaniam. MD, DM. Resident Director. Kidney Care Centre. Tirunelveli. Tamilnadu, India.
Comment of the reviewer Jesús Garrido, MD. Unidade de Nefrologia e Diálise. Hospital São Teotónio de Viseu. Viseu. Portugal
SUMMARY
Acute renal failure is a syndrome that usually runs with an increase in creatinine and urea plasma levels. However, there are clinical situations in which this syndrome may run with an increase in plasma creatinine keeping normal the urea one. In this report we present a case of acute renal failure with normal plasma urea level secondary to an acute pyelonephritis in a single kidney patient. The patient had an increased fractional excretion of urea which could explain the normal plasma urea levels found despite of his reduced glomerular filtration. This increased urea excretion state was interpreted as a consequence of the nephrogenic diabetes insipidus and alteration of the intra-renal urea reciclying process that the acute pyelonephritis induced. In conclusion: Acute pyelonephritis in a single kidney patient can appear as a pattern of acute renal failure with normal plasma urea levels.
KEY WORDS: acute renal failure, normal uremia, acute pyelonephritis
RESUMEN
La insuficiencia renal aguda es un sindrome que característicamente cursa con niveles plasmáticos elevados de urea y creatinina. Sin embargo, hay situaciones clínicas en las cuales este sindrome puede cursar con un incremento de la creatininemia sin presentar elevación de la uremia. En este reporte presentamos un caso clínico de una insuficiencia renal aguda con uremia normal secundaria a una pielonefritis aguda en un paciente con riñón único. El paciente presentaba una elevada excreción fraccional de urea lo cual podía explicar su uremia normal pese a estar cursando una caída del filtrado gomerular. Dicha excreción de urea elevada fue interpretada como secundaria a una diabetes insipida nefrogénica y una alteración en el recirculado intra-renal de la urea ambos producto de la pielonefritis aguda. Concluimos que la pielonefritis aguda en un paciente mono-reno puede presentarse con un patrón de insuficiencia renal aguda con uremia normal.
PALABRAS CLAVE: Insuficiencia renal aguda, uremia normal, pielonefritis.
INTRODUCTION
Acute renal failure is a syndrome that usually runs with an increase in creatinine and urea plasma levels since in both substances the glomerular filtration plays an important role in their excretion1.
However, there are clinical situations in which an acute renal failure may run with an increase in plasma creatinine keeping normal the urea level. Examples of the afore mentioned clinical situations are those patients who suffer from acute renal failure in the context of low protein intake, hepatic insufficiency, or/and diabetes insipidus2-4.
In the following report we present a case of acute renal failure with normal plasma urea level secondary to an acute pyelonephritis in a single kidney patient.
CASE REPORT
Male patient, sixty-two years old who suffered from the following diseases: Diabetes mellitus (type II) treated with diet and 4 mg/day of glymepiride. Right nephrectomy performed ten years before due to uropyonephrosis. Urolithiasis (in the past). Hypercholesterolemia treated with sinvastatin (10 mg/day) and ezetimibe (10 mg/day)
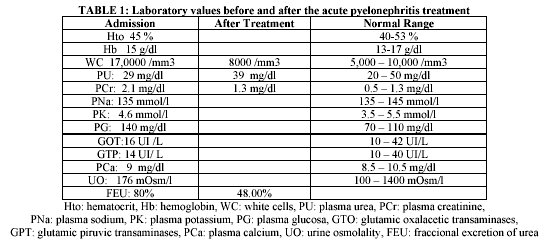
He was admitted in our hospital presenting two day of evolution of a left lumbar pain, dysuria, and fever. Blood and urine laboratories were performed. Abundant leucocytes and pyocytes were documented in the urinalysis, while reduced creatinine clearance (35 ml/minute), normal plasma urea (29 mg/dl) and increased plasma creatinine (2,1 mg/dl) and fractional excretion of urea (80%) were detected.
The patient presented water polyuria (urine volume: 3000 cc with urine osmolality: 176 mOsm/l), slightly increased plasma glucose (130 mg/dl) and normal plasma sodium (135 mmol/l) levels.
The patient was not under any nephrotoxic drug and he had no clinical or laboratory evidence of rhabdomyolysis. He did not suffer from any disease that could reduce his plasma urea level such as malnutrition, hepatic disease or Fanconi syndrome.
The case was interpreted as an acute renal failure secondary to acute pyelonephritis in a single kidney patient. After blood and urine cultures were obtained intravenous ceftriaxone (2 gr/day) was initiated. Urine culture was positive to Escherichia coli sensitive to the prescribed antibiotic.
After the infection was cured the fractional excretion of urea (48%), plasma creatinine (1.3mg/dl), creatinine clearance 110 ml/minute and plasma urea (39) levels reached their usual values (Table 1).
DISCUSSION
Urea is the major end product of protein catabolism in mammals. It is synthesized in the liver and excreted mainly by the kidney. Under basal conditions, this substance has a glomerular filtration of 100 % although its final excretion is around 50%. This lower excreted amount respect to the filtrated one is a consequence of its reabsorption in the proximal tubules and in the very late part of the collecting ducts, close to the papillary tip. Moreover, since urea is also secreted in the S3 segment of proximal tubules, this substance suffers an intra-renal recycling process which contributes to reduce its excretion5-6.
Acute renal failure syndrome usually runs with an increase in creatinine and urea plasma levels since in both substances glomerular filtration plays an important role in their excretion1.
However, there are situations of acute renal failure with increased plasma creatinine levels but normal urea ones. This phenomenon can be justified mainly by two physio-pathologic mechanisms:
In our reported case it can delineate three syndromes:
CONCLUSION:
Acute pyelonephritis in a single kidney patient can appear as a pattern of acute renal failure with normal plasma urea levels.
REFERENCES
- 1.- Tovar JL, Pascual J, Liaño F. Diagnóstico diferencial del fracaso renal agudo. In Liaño F, Pascual J. Fracaso renal agudo. Barcelona. Masson. 2000: 103-125
2.- Faber M, Kupin W, Krishna, Narins R. The differential diagnosis of acute renal failure. In Lazarus JM, Brenner BM. Acute renal failure. New York. Churchil Livingstone. 1993: 133-192
3.- Bataller R, Arroyo V. Fracaso renal agudo asociado a enfermedades hepáticas. Síndrome hepatorenal. In Liaño F, Pascual J. Fracaso renal agudo. Barcelona. Masson. 2000: 103-125:313-326
4.- Musso CG, Giordani C, Stonski E, Peralta M, Bonetto A, Jauregui R, Algranati L. Acute renal failure with normal plasma urea levels: a marker proximal tubular disfunction with diabetes insipidus. Rev Electron Biomed / Electron J Biomed 2004;2:65-68
5.- Bankir L, Trinh-Trang-Tan M. Urea and the kidney. In Brenner B, The Kidney. Philadelphia. W.B. Saunders. 2000: 637-679
6.- Robertson G, Berl T. Pathophysiology of water metabolism. In Brenner B, The Kidney. Philadelphia. W.B. Saunders. 2000: 1996: 873-928
7.- Andriole V. Urinary tract infections and pyelonephritis. In Wyngaarden J, Smith LL, Bennett JC. (Eds). Cecil Textbook of Medicine. W. B. Saunders. 1995: 593-598.
8.- Gilbert RM, Weber H, Turchin L, Fine LG, Bourgoignie JJ, Bricker NS. A study of the intrarenal recycling of urea in the rat with chronic experimental pyelonephritis.Clin Invest. 1976 58(6): 1348-1357.