Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
TOURNIQUET: LACUNAE OF PREANALYTICS
Smita S. Sonoli MD, Anuradha B. Patil MD, P. B. Desai MD,
M. V. Kodliwadmath MD, C. V. B. Prasad PhD, Shivprasad MD.
Department of Biochemistry,
KLE University's Jawaharlal Nehru Medical College.
Belgaum, Karnataka, India.
drsmitasonoli @ yahoo.co.in
Rev Electron Biomed / Electron J Biomed 2009;2:56-61
Comment of the reviewer Pilar Calmarza, PhD. Laboratorio de Bioquímica. Hospital Miguel Servet. Zaragoza. España.
Comment of the reviewer Dra. Pilar García-Chico Sepúlveda. Jefe del Servicio de Análisis Clínicos del Hospital General de Ciudad Real. España.
RESUMEN:
Objetivo: Este estudio tuvo como objetivo investigar la influencia del estancamiento prolongado, creado durante la recogida de la muestra de sangre, sobre cinco parámetros bioquímicos comunes.
Metodología: La sangre fue recogida por punción venosa de 20 individuos sanos. Cinco muestras fueron recolectadas, una antes de aplicar presión y cuatro después de aplicar presión estándar de 60 mm de Hg (1 y 3 minutos) y 90 mm de Hg (1 y 3 minutos) con la ayuda del esfingomanómetro. Los valores de proteínas totales, albúmina, glucosa, urea y creatinina se calcularon por el método de kit y análisis en un semiautoanalizador, fabricado por Transasia en colaboración con Erba Diagnostic (Alemania).
Resultados: No hubo aumento en los niveles de proteínas totales y albúmina y la disminución de los niveles de glucosa y urea (p <0,05) con aumento de la presión y el tiempo. Sin embargo, la creatinina no mostró cambios en los valores de estancamiento a corto plazo, pero la estasis prolongada a 90 mm de Hg durante 3 minutos mostró una disminución en los valores (p <0,02).
Conclusión: A partir de nuestros resultados, podemos concluir que los parámetros en cuestión son influenciados por la duración y la magnitud de la presión aplicada, por lo tanto, el torniquete se debe utilizar de manera meticulosa. El personal del Laboratorio debe ser educado sobre el uso de torniquete, para que los errores de laboratorio puedan ser identificados y prevenidos.
PALABRAS CLAVE: Errores preanalíticos. Estasis prolongado. Flebotomía. Torniquete.
SUMMARY:
Aim / Objective: This study was aimed to investigate the influence of prolonged stasis, created during blood sample collection, on five common biochemical parameters.
Methodology: Blood was collected by venepuncture from 20 healthy individuals. 5 samples were collected. One before applying standard pressure and four after applying standardized pressure of 60 mm of Hg(1 and 3 minutes) and 90 mm of Hg (1 and 3 minutes) with help of sypgmomanometer. Total protein, albumin, glucose, urea, creatinine were estimated by kit method and analysed on semiautoanalyzer manufactured by Transasia in collaboration with Erba Diagnostics (Germany).
Results: There was increase in the levels of total protein and albumin and decrease in levels of glucose and urea (p <0.05) with increase in pressure and time. However creatinine did not show change in values on short term stasis, but prolonged stasis at 90 mm of Hg for (3 minutes) showed decrease in values (p < 0.02).
Conclusion: From our results, we conclude that the parameters in question are influenced by the duration and magnitude of pressure applied, hence tourniquet should be used meticulously. Phlebotomists should be educated regarding the usage of tourniquet so that laboratory errors can be identified and prevented.
KEY WORDS: Phlebotomy. Pre-analytical errors. Prolonged stasis. Tourniquet.
INTRODUCTION
Quality assurance is the focus of current concern in laboratory, as laboratory errors are of great impact on medical diagnosis and therapies. Errors might originate from pre analytical, analytical and post analytical sources, hence laboratorians have realised the importance of monitoring all the steps in laboratory tests to detect and prevent defects.
Advances in instrument technology and automation have simplified tasks in laboratory diagnostics and improved the quality of test results, thereby decreasing the analytical defects to less than 7-10%1. Improvement now should be targeted to extra-analytical phase (pre analytical and post analytical phase). However difficulties to monitor the pre analytical variables are that, they lie outside the direct control of laboratory personnel, one such being phlebotomy. In developing countries like India, there is lack of understanding about good laboratory practices and inadequate training to phlebotomists, compelling them to make errors during phlebotomy. The improper venous accesses, or prolonged venous stasis created by tourniquet application will result in collection of unsuitable blood sample.
Ideally, the tourniquet should be used only if necessary and removed as soon as the needle is within the vein. A normal healthy individual with a systolic blood pressure of 120-130 mm of Hg, the pressure from the tourniquet should be around 100 mm of Hg and should not last longer than 1 minute2. Unfortunately this is never practised; the amount of time and pressure created by tourniquet is often under looked by the phlebotomist leading to prolonged stasis, and the amount of pressure far exceeds, which may reach up to 90-100 mm of Hg, or even more which is never analysed.
Keeping this in view, the aim of our study, was to assess the effect of prolonged stasis created by sypgomanometer of about 60 mm of Hg(1 and 3 minutes) and 90 mm of Hg (1 and 3 minutes) on five biochemical parameters routinely done in all laboratories.
MATERIAL AND METHODS
The Study was conducted in Department of Biochemistry, Jawaharlal Nehru Medical College, Belgaum.
Inclusion Criteria:
20 healthy males in the age group of 28 to 32 years were selected as participants of this study. Morning fasting sample was taken using 21 gauge straight needle and collected in vacutainer by single experienced ,expert phlebotomist using same sphygmomanometer every time to create the required standardized pressure. Sphygmomanometer mimicked as tourniquet. The study was approved by Ethical Committee of the Jawaharlal Nehru Medical College, Belgaum. Consent was taken from all participants.
Exclusion Criteria:
Elderly males, children, obese individuals, smokers, alcoholics and individuals with systemic diseases were excluded from this study.
Procedure for Blood Collection:
All Samples were collected in sitting position. Venipuncture was done on different arms of anticubital site to exclude any interference originating from the previous tourniquet. The first phlebotomy was carried out without stasis, while the subsequent four with stasis. Second and third samples were collected after application of standard external pressure of 60 mm of Hg using sphygmomanometer for one and three minutes while fourth and fifth samples were collected after application of standard external pressure of 90 mm of Hg for 1 and 3 minutes. The pressure was released only after the blood was drawn and after every prick rest time of 10 min was given to the volunteers. 3 ml of Blood was collected every time out of which 2 ml was evacuated into the vacuum tube containing gel of the same lot and 1 ml was collected in fluoride containing tubes for analysis of glucose.
Serum was obtained after allowing it to clot for 30 minutes at room temperature, followed by centrifugation at 3000 rpm for 10 minutes. All Specimens were processed within 2 hours of collection. Total protein, albumin, glucose, urea, creatinine were estimated by kit method and analysed on semiautoanalyzer manufactured by Transasia in collaboration with Erba Diagnostics (Germany).
The Instrument was calibrated against appropriate reference standard material & controlled daily by the use of control sera, there by maintaining Quality control.
Statistical Analysis: The data were expressed as mean ± standard deviation (M ± SD). Student 't' test was used to detect significant differences between no stasis and other groups. The difference was considered significant at p < 0.05.
RESULTS
Results of our present evaluation are summarized in Table 1.
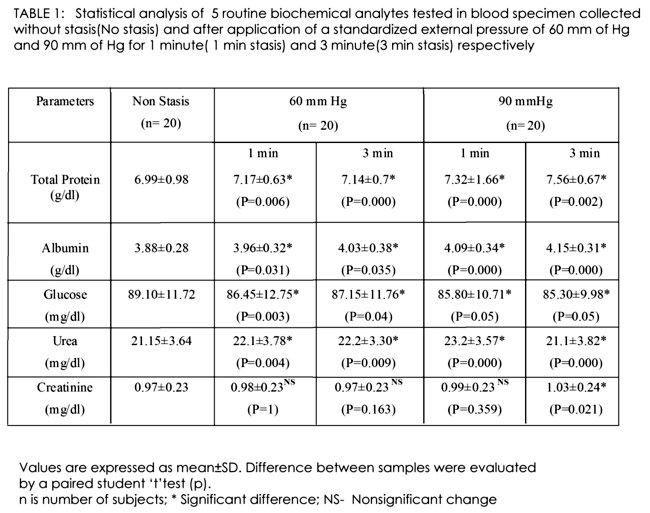
Statistically significant differences according to the paired student 't'- test could be observed between the samples collected with stasis after a standardized pressure of 60 mm and 90 mm of Hg was applied for 1 and 3 minutes with that of Non stasis(p<0.05).
Although statistical analysis was satisfactory for total protein, albumin, glucose and urea, the clinical acceptability was somehow lower for creatinine.
DISCUSSION
Today's era of modern medicine focuses to achieve total quality in laboratory testing. Earlier investigations which have surveyed the causes of laboratory errors found that out of total error, 46% are contributed by pre-analytical phase, 47% by post-analytical & 7% by analytical3. To err is human, but to persevere in error is only the act of a fool. This is also reasonably true when dealing with laboratory errors, unless such errors can actually be identified4 and rectified. Only awareness of the mistake is not enough, vigorous steps to reduce them is mandatory, to improve the overall quality of laboratory services.
In course of time analytical errors have been reduced drastically. So our prime focus being pre-analytical phase. Phlebotomy, is one of the pre-analytical phase, which is least supervised. Although there are standard guidelines, for blood sample collection, but none are mandatory in India5, leading to errors by phlebotomist. Errors are due to their ignorance about the methods of sample collection as they are lacking proper education regarding the standard guidelines. Actually, tourniquet should be used only in cases of non accessibility of veins. But, tourniquet is tied before the blood is drawn and till the blood is drawn, immaterial of veins visibility and without accessing the amount of time and pressure being created by it. So keeping these observations in view, in our study we have created both short term venous stasis and prolonged stasis, for blood sample collection.
We analysed that there was statistical significant difference(P<0.05) between the samples collected by without stasis and with stasis of 60 and 90 mm of Hg for 1 & 3 minutes respectively created by sphygmomanometer in cases of 4 parameters those are total proteins, albumin, glucose and urea. Total protein and albumin levels increased with increase in pressure. While glucose and urea level decreased with increase in pressure.
The result is in accordance with study done by Lippe G et al6. Contradictory results have been observed by Mc Mullan et al7, Jung B et al8, McNair P et al9 and Serdar MA et al10. In our study in case of creatinine, statistically significant difference (P<0.02) between the sample collected by non stasis and with stasis at 90mm of Hg for 3 minute was observed, but no statistical significant difference between the sample collected at 1 & 3 minutes for 60mm of Hg and 1 min for pressure of 90mm of Hg with that of non stasis was observed. This result shows that, short term venous stasis has no effect on creatinine values, but long term do has attributed to the extravasation of creatinine from the strained localised muscle tissue11 caused by tourniquet application.
Hypothesis states that the application of tourniquet, by reducing pressure below systolic pressure, maintains the effective filtration pressure within the capillaries. As a result, small molecules and fluid are transferred from intravasal space to the interstitium. Application of the tourniquet for longer than 1 minute and up to 3 minute can result in hemoconcentration, causing an increase in the concentration of large molecules that are unable to penetrate the capillary wall12. However this hypothesis does not hold good for creatinine in our study.
We can conclude from our study that application of tourniquet for a prolonged time influences the reliability of the results, for instance, glucose levels keep on decreasing with increase in pressure, then there are chances of missing cases of borderline diabetes mellitus. Urea level decreased with increase in pressure, and then we may faultily report a renal diseased person to be in a recovery state. So one of the remedial measure to access the amount of time and pressure created is usage of re/de-inflatable devices as suggested by Lippi G et al6. Even we can formulate some correction factors for the parameters showing changes with change in pressure as one being done for the estimation of calcium by Mc Mullan et al7.
Our suggestion are manufacturing of new type of tourniquet which can show pressure changes digitally, when applied. Better is to avoid tourniquet, when not required, as in case of visible veins. Lastly, phlebotomists have to be educated regarding the proper and timely usage of tourniquet. However further studies have to be done with a larger sample size and involvement of patients with diseases to see the changes in the levels of parameter in question.
CONCLUSION
Results from our investigation, confirms that, the biochemical parameters, tend to vary with change in duration and pressure created by tourniquet. Just awareness is not enough, but vigorous action to reduce the errors is mandatory.
REFERENCES
- 1.- Plebani M. Errors in clinical laboratories or errors in laboratory medicine? Clin Chem Lab Med 2006; 44: 750-759.
2.- Dittmann M. Blood collection techniques. An Informative guide to blood collection 6th edition. Greiner Bio-One GmpH, Kremsmunster Austria 2008: 1-24.
3.- Plebani M, Carraro P. Mistakes in a stat laboratory:types and frequency. Clinical Chem 1997 Aug; 43(8 Pt 1):1348-1351.
4.- Lippi G, Guidi GC, Mattiuzzi C, Plebani M. Preanalytical variability: the dark side of the moon in laboratory testing. Clin Chem Lab Med 2006; 44: 358-365.
5.- Ashavaid TF, Dandekar SP, Keny B, Bhambhwani VR. Influence of blood specimen collection method on various preanalytical sample quality indicators.Indian J Clin Biochem 2008; 23: 144-149.
6.- Narayanan S. The Preanalytic Phase- An Important Component of Laboratory Medicine. Am J Clin Pathol 2000; 113: 429-452.
7.- Lippi G, Salvagno GL, Montagnana M, Brocco G, Guidi GC. Influence of short-term venous stasis on clinical chemistry testing. Clin Chem Lab Med 2005; 43: 869-875.
8.- McMullan AD, Burns J, Paterson CR. Venepuncture for calcium assays: should we still avoid the tourniquet? Postgrad Med J 1990; 66: 547-548.
9.- Junge B, Hoffmeister H, Feddersen HM, Rocker L. Standardisation of obtaining blood samples: influence of tourniquet application on 33 constituents of blood and serum. Dtsch Med Wochenschr 1978; 103: 260-265.
10.- McNair P, Nielsen SL, Christiansen C, Axelsson C .Gross errors made by routine blood sampling from two sites using a tourniquet applied at different positions. Clin Chim Acta. 1979; 98(1-2): 113-118.
11.- Young DS, Bermes Jr. EW. Preanalytical variables and biological variation. Tietz Text Book of Clinical Chemistry and Molecular Diagnostics 4th edition. Elsevier, New Delhi 2006: 449-473.
12.- Serdar MA, Kenar L, Hasimi A, Kocu L, Türkmen YH, Kurt I, Akman S , Erbil Mk. Tourniquet Application Time During Phlebotomy and TheInfluence on Clinical Chemistry Testing; Is It Negligible? Turkish J Biochem 2008; 33: 85-88.
CORRESPONDENCE:
Dr. Smita S. Sonoli
Assistant Professor. Department of Biochemistry
Jawaharlal Nehru Medical
Nehru nagar. Belgaum- 590 010
Karnataka, INDIA
E mail: drsmitasonoli @ yahoo.co.in
The pre-analytical phase is a vitally important part of the process for accurate results in any biochemical analysis.
A large number of errors can occur within the wide spectrum of this phase, and knowledge of them and their detection is the responsibility of the clinical laboratory professionals.
Although there are many studies on the quality of the analytical phase in clinical analysis, the same cannot be said of the pre-analytical and post-analytical phases. This may be because their great importance in the final result of the biochemical analysis has only been recently recognised.
It is the responsibility of the laboratory to take the necessary measures to minimise the sources of error in the pre-analytical phase, in aspects regarding the correct filling in of the analysis request form, as well the correct drawing and collection of the sample, developing standard procedures for preparation of the patient and obtaining the sample.
As regards obtaining the blood sample, as is demonstrated in this work, the time of applying the tourniquet is fundamental, attempting to minimise its use as far as is possible.
The standardisation of all these parameters will lead to a higher quality of the analytical process itself; this process being considered as a single entity which in turn consists of the pre-analytical, analytical and post-analytical phases.