Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
CLINICAL STUDY OF THE CHRONOLOGICAL
CHANGES IN KNEE ALIGNMENT PATTERN
IN NORMAL SOUTH-EAST NIGERIAN CHILDREN
AGED BETWEEN 0 AND 5 YEARS
Ezeuko V.C, Owah S, Ukoima H.S, Ejimofor O.C, Aligwekwe A.U, Bankole L.
Department of Anatomy, Faculty of Basic Medical Sciences.
Madonna University, Elele Campus, Rivers State.
Nigeria
chuksy4love2001 @ yahoo.com
Rev Electron Biomed / Electron J Biomed 2010;1:16-21
Comment of the reviewer Prof. Mario Arturo González-Marińo MD. Professor of Epidemiology, College of Medicine. Fundación Universitaria San Martín. Bogotá, Colombia.
Comment of the reviewer José Luis Hernández Cáceres PhD. Center for Cybernetics Applications to Medicine (CECAM). Havana, Cuba.
ABSTRACT
The purpose of this study is to establish the chronological changes in knee alignment pattern in normal South-East Nigerian children aged between 0 and 5 years. A total number of 1450 subjects (680 males and 770 females) were used for the study. The intercondylar/intermalleolar distances were measured using a vernier caliper with the subjects standing erect in anatomical position to determine straight knee, genu valgum and genu varum. The data was analysed with Microsoft Excel version 2007. The prevalence was presented as percentage (%).
The result showed that the subjects have varum by the first year of life, prevalently genu valgum in type by the second year, valgum by the third year, neutral by the fourth and fifth year.
Keywords: Knee alignment patterns, genu varum, genu valgum, South-East Nigeria
RESUMEN
El propósito del presente estudio ha sido determinar los cambios cronológicos en el patrón de alineamiento de las rodillas de nińos normales procedentes del sudeste de Nigeria entre 0 y 5 ańos de edad. El estudio incluyó un total de 1450 sujetos (680 nińos y 770 nińas). Se utilizó un calibrador anatómico para medir las distancias intercondilar e intermaleolar estando el sujeto en posición anatómica erecta, lo que permitía decidir si el sujeto presentaba alineamiento recto de las rodillas o si debía clasificarse como genu valgum y genu varum.
Para el análisis de los datos se utilizó el programa Microsoft Excel versión 2007. La prevalencia se expresó en porcentajes (%).
Se obtuvo que entre los sujetos prevalecía genu varum durante el primer ańo de vida, genu valgum durante el segundo ańo, valgum al tercer ańo y neutral al cuarto y quinto ańos de vida.
Palabras clave: Datos cronológicos. Alineación de la rodilla. Genu valgum. Genu varum Sudeste de Nigeria.
INTRODUCTION
The bowleggedness and knock-knees are frequently encountered angular deformities in pediatric orthopaedic clinics. Although benign and self-limiting in most cases, these deformities sometimes cause a great concern to the parents and the relatives1-6, and such anxieties frequently lead physicians to conduct physical or radiological examinations4,7-9. However, even after these examinations have been conducted, misunderstandings of physiologic ranges and changes in knee alignment might initiate costly and time-consuming therapeutic measures, such as, bracing, which may be entirely unnecessary and in certain instances may prove harmful8.
Genu valgum, commonly called "knock-knees", is a condition where the knees angle in and touch one another when the legs are straightened. Females have a wider pelvis than men and a relatively shorter length of the thigh bone, and as a result, have a greater static genu valgum than men. Individuals with severe valgus deformities are typically unable to touch their feet together while simultaneously straightening the legs.
Genu varum (also called bow-leggedness or bandiness), is a deformity marked by medial angulation of the leg in relation to the thigh, an outward bowing of the legs, giving the appearance of a bow. Usually there is an outward curvature of both femur and tibia. Genu varum is a relatively common finding in children. Physiologic bowing, which is seen most often, has a well-documented favorable natural history. Children until the age of 3 to 4 have a degree of Genu varum.
The child lies on its nurse's knee with the soles of the feet facing one another; the tibia and femur are curved outwards; and, if the limbs are extended, although the ankles are in contact, there is a distinct space between the knee-joints. During the first year of life a gradual change takes place. The knee-joints approach one another; the femur slopes downward and inward towards the knee joints; the tibia become straight; and the sole of the foot faces almost directly downwards. While these changes are occurring, the bones, which at first consist principally of cartilage, are gradually becoming ossified. By the time a normal child begins to walk the lower limbs are prepared, both by their general direction and by the rigidity of the bones which form them, to support the weight of the body.
Many studies have established that the tibiofemoral (TF) angle changes in healthy growing children. It may be expressed in degrees or as centimetres of either the intermalleolar (IM) or the intercondylar (IC) distance. The normal range of TF angle, calculated as two standard deviations (SD) about the mean, for normal children between birth and 12 years of age has been reported clinically7-8 and radiologically10.
It has been well established by previous studies involving radiological analysis and clinical measurements that children undergo sequential physiologic changes in axial alignment, i.e., genu varum, neutral, and genu valgum, during normal development4-5,7-8,10. Moreover, the physiologic changes in knee angle have been investigated with respect to gait, joint range of motion, and torsional deformities4-5, and have been found to correct spontaneously in time3-4,10. However, the absence of values defining normal ranges in different ethnic groups limits the application of this information11.
In Nigeria, at least two published works from Western and Northern parts with different diets and cultural practices, found different varieties of angular deformities around the knee12-13.
Omololu13 agreed that clinical evaluation is reliable and reproducible enough for day-to-day practice, but there are insufficient data for children between 0 and 10 years of age. In this period, knowledge of normal data is important to differentiate between physiological variation and pathological deformity which may require further evaluation and treatment. There is little data on the range of variation of knee angle, intermalleolar and intercondylar distances in African children13.
This is study is thus purposed to establish a chronological data on the normal development of knee alignment among children of South-East Nigeria aged 0-5 years.
MATERIALS AND METHODS
Subjects /Study population
A total number of 1450 subjects, whose parents or guardians gave their consent, were used for the study made up of 680 males and 770 females with their age ranging between 0 and 5 years. The subjects selected for the study were strictly South-East Nigerian based on the origin of parents and grand parents. All cases of abnormalities related with the lower limb were excluded from the study. The subjects were grouped into 5 according to the age. Group A aged between 0 and 1 year, group B aged greater than 1 year but less than or equal to 2 years, group C aged greater than 2 years but less than or equal to 3 years, group D aged greater than 3 years but less than or equal to 4 years, group E aged greater than 4 year but less than or equal to 5 years.
Measurement techniques
With the subjects standing erect in anatomical position with the hip and knee in maximum extension and lower limbs together so that the two medial femoral condyles and/or the two medial malleoli touch. Toddlers were allowed to lie in supine position. The intercondylar/intermalleolar distances were measured using a vernier caliper. Intermalleolar distance is the distance between the right and left medial malleoli while intercondylar distance is the distance between the right and left medial femoral condyles.
The knee alignment was considered to be neutral when there is no demonstrable intercondylar distance and there is also no demonstrable intermalleolar distance.
The knee alignment was considered to be varus when there is a demonstrable intercondylar distance while the two medial malleoli are touching.
The knee alignment was considered to be valgus when there is a demonstrable intermalleolar distance while the two medial femoral condyles are touching.
Statistical analysis
The data was analysed with Microsoft excel version 2007. The prevalence was presented as percentage (%).
RESULTS

Figure 1: Bar chart showing prevalence of knee angle type among different age groups
From figure 1 above, out of the 306 subjects in group A, none had straight limbs (NT), 306 (100%) had genu varum (VR) while none had genu valgum (VL). Out of the 314 subjects in group B, none had straight limbs (NT), 62 (19.75%) had genu varum while 252 (80.25%) had genu valgum (VL). Out of the 274 subjects in group C, none had straight limbs (NT) , none had genu varum while 274 (100%) had genu valgum (VL). Out of the 284 subjects in group D, 282 (99.30%) had straight limbs (NT) , none had genu varum while 2 (0.70%) had genu valgum (VL). Out of the 272 subjects in group E, 272 (100%) had straight limbs (NT) , none had genu varum and none had genu valgum (VL).
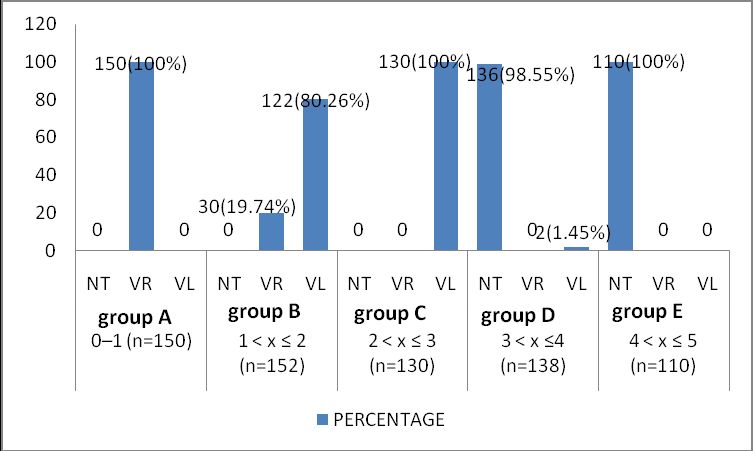
Figure 2: Bar chart showing prevalence of knee angle type among different age groups in males groups
From figure 2 above, out of the 150 male subjects in group A, none had straight limbs (NT) , 150 (100%) had genu varum while none had genu valgum (VL). Out of the 152 male subjects in group B, none had straight limbs (NT) , 30 (19.74%) had genu varum while 122 (80.26%) had genu valgum(VL). Out of the 130 male subjects in group C, none had straight limbs (NT) , none had genu varum while 130 (100%) had genu valgum(VL). Out of the 138 male subjects in group D, 136 (98.55%) had straight limbs (NT) , none had genu varum while 2 (1.45%) had genu valgum(VL). Out of the 110 male subjects in group E, 110 (100%) had straight limbs (NT) , none had genu varum and none had genu valgum(VL).
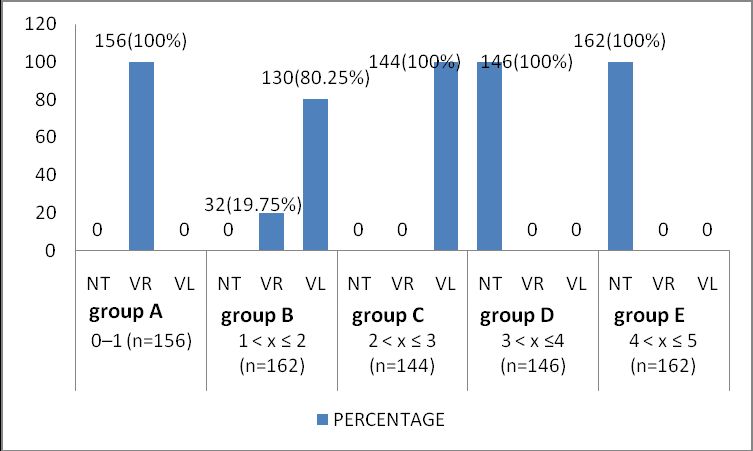
Figure 3: Bar chart showing prevalence of knee angle type among different age groups in females groups
From figure 3 above, out of the 156 female subjects in group A, none had straight limbs (NT) , 156 (100%) had genu varum while none had genu valgum (VL). Out of the 162 female subjects in group B, none had straight limbs (NT) , 32 (19.75%) had genu varum while 130 (80.25%) had genu valgum (VL). Out of the 144 female subjects in group C, none had straight limbs (NT) , none had genu varum while 144 (100%) had genu valgum (VL). Out of the 146 female subjects in group D, 146 (100%) had straight limbs (NT) , none had genu varum (VR) while none had genu valgum (VL). Out of the 162 female subjects in group E, 162 (100%) had straight limbs (NT) , none had genu varum (VR) and none had genu valgum (VL).
DISCUSSION
The establishment of a normal range of knee alignment in children is of paramount clinical importance, as such knowledge would allow physicians to determine whether the knee alignment in a specific patient represents physiologic development or not. Moreover, a relevant and correct understanding of the development of the knee angle and limb alignment would prevent unreasonable apprehension by parents and relatives, and unnecessary diagnostic measurements, such as repeated exposure to radiation, and the inappropriate application of orthotics or bracing, which are not often cost-effective and might hinder natural development6-8. In addition, this understanding would help diagnose, evaluate, and treat pathologic conditions, such as infantile tibia vara or Blount disease1,3,6.
Several authors, based upon clinical measurements and radiological analyses, have reported on the development of knee angle in children. Salenius and Vankka10 were the first to investigate the development of the knee angle radiologically. Yoo et al11 studied the development of tibiofemoral angle in Korean children radiologically and showed patterns of sequential physiologic knee angle changes that are similar to those reported in other races4-5,7-8,10 although the valgus peak occurred later and the overall development more prolonged.
In summary, this study provided the data of the chronological changes of the lower limb alignment for the South-East Nigerian children by clinical measurements. The overall pattern of chronological changes in the knee angle or the anatomical tibiofemoral angle was similar to those found in other ethnic groups i.e. varum by the first year of life, prevalently genu valgum in type by the second year, valgum by the third year, neutral by the fourth and fifth year. Earlier work by Greenberg and Swartz14 found the peak incidence of genu varum (VR) to be between 1 and 2 years of age, while that of genu valgum was found to be between the ages of 3 and 4 years in this population. This shows a slight earlier transition of the knee angulation in South-East Nigerians. This could however be as a result of the long interval between the two studies.
These normative data should be taken into consideration when evaluating lower limb alignment in children.
One should be cautious when describing what is 'normal', because of possibilities of individual and ethnic variations. Although Cheng et al8 concluded that trends in the Chinese were nearly identical to those shown in other races in this context, Heath and Staheli7 suggested that there are racial differences. Whereas Cheng et al8 concluded that soon after three years of age, the tibiofemoral angle of Chinese children approaches 0o, which indicates that the normal Chinese children aged between 3 and 11 years exhibit a significant amount of varus, Heath and Staheli7 observed preservation of valgus with a mean of 2.8o at 11 years, and normal limits of these ages did not include any amount of varus, hence more varus in Chinese children than in white children.
REFERENCES
-
1. McDade W. Bowlegs and knock knees. Pediatr Clin North Am. 1977; 24: 825-839
2. Morley AJ. Knock knee in children. Br Med J. 1957; 2(5051): 976-979
3. Sherman M. Physiologic bowing of the legs. South Med J. 1960; 53: 830-836
4. Engel GM, Staheli LT. The natural history of torsion and other factors influencing gait in childhood. A study of the angle of gait, tibial torsion, knee angle, hip rotation, and development of the arch in normal children. Clin Orthop Relat Res 1974; 99:12-17
5. Hachiya MA. Roentgenographical study on chronological changes in genu varum and valgum in children (author's transl). Nippon Seikeigeka Gakkai Zashi 1981; 55(1): 31-43
6. Levine AM, Drennan JC. Physiological bowing and tibia vara. The metaphyseal-diaphyseal angle in the measurement of bowleg deformities. J Bone Joint Surg Am 1982; 64: 1158-1163
7. Heath CH, Staheli LT. Normal limits of knee angle in white children - genu varum and genu valgum. J Pediatr Orthop 1993; 13: 259-262
8. Cheng JC, Chan PS, Chiang SC, Hui PW. Rotational profile of the lower limb in 2,630 Chinese children. J Pediatr Orthop 1991; 11: 154-161
9. Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am 1987; 69: 745-749
10. Salenius P, Vankka E. The development of the tibiofemoral angle in children. J Bone Joint Surg Am 1975; 57: 259-261
11. Yoo JH, Choi IH, Cho T, Chung CY, Yoo WJ. Development of Tibiofemoral Angle in Korean Children. J Korean Med Sci 2008; 23 : 714-717
12. Solagberu BA. Angular deformities of knee in children. Nigerian J Surg Res 2000; 2: 62-67
13. Omololu B, Tella A, Ogunlade S.O, Adeyemi AA, Adebisi A, Alonge TO, Salawu SA, Akinpelu AO. Normal values of knee angle, intercondylar and intermalleolar distances in Nigeria children. West Afr J Med 2003; 22 (4): 301-4
14. Greenberg LA, Swartz AA. genu varum and genu valgum. Am J Dis 1971; 121 : 219-221
Correspondence:
Ezeuko V.C
Department of Anatomy, Faculty of Basic Medical Sciences.
Madonna University. Elele Campus
Rivers State. Nigeria
Mail: chuksy4love2001 @ yahoo.com