Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
- Research: in this category some of the parameters that are included are: number of projects, number of researchers, research funds, agreements with companies, number of original and review articles, impact factor, communications to congresses, patents, etc One of our own indicators included in this section is the economic value of impact factor.
- Teaching: in this section some of the indicators that are included are: the number of medical residents and staff in training, courses and seminars given, etc As an example of own indicator, we have included the number of courses and congressed attended by our residents and the staff in training
- Other merits: Awards received, media interviews, etc As an own indicator, the number of meetings done by a research group during a period of time is included
- Personnel: This module allows storing and managing the research staff CV. It also allows the user to identify the right specialist for a specific task, and browse a researcher's web-based curriculum vitae. Furthermore, it is possible to view the research activity for a particular researcher (his/her publications, his/her projects underway, the type and duration of his/her contract, or his/her dedication to the different projects to avoid incompatibilities).
- Projects: This module enables users to learn about the research goals of our institute through its past and current projects. A visitor to a project's web page can view the CVs of researchers working on that project and all publications related to the project as well as other relevant information about this project (legal and financial information, etc) .
- Publications: This module provides access to indexed references of publications (technical reports, theses, conference papers, journal articles) authored by our researchers, with links to the full-text original documents whenever possible. Publications can be sorted by a researcher, or a research group, or a project or in general by a period of time.
- News board: This module allows accessing all relevant information about relevant topics such as calls for proposals announcements or meetings, etc. Our tool allows the entry all of the information needed to be able to manage official announcements of research aid. Later, the applications researchers complete for each one of the official announcements may be stored. When the application is submitted for an official announcement, the researcher may report the detailed budget for the aid being requested. When reporting the aid data, data may be taken from the application or the aid may be entered from scratch. When entering the aid, all the financial data for the aid granted is reported with a breakdown of the budget by items and accounting periods. Once the aid data has been entered, it is possible to financially monitor the income, expenses and justifications through a gateway to the budget accounting application. This is part of the project module.
- Diary: This module is used for managing all information about the meetings. It can be public or private. Public means that all researchers can access to it. It contains information about the research meetings (calls, documentation, minutes, etc). The private diary can be used by a research group or a researcher to organize his/hers own meetings.
- Reports: This module allows to automatically obtain our annual report based on the scientific activities entered within the rest of the modules. It also allows obtaining the information in different periods (two-year, five-year period, etc)
- The Director of the ICICOR who is the main responsible for the development of the research area at the ICICOR.
- The Research Committee which is formed by the Director, each Research area Coordinator, the Tutor of the Medical Residents, the Chief of the Cardiac Surgery Department, and the Research Coordinator. Its main responsibilities are to approve new research areas or to close down some old ones, to
- The Research Support Unit which is formed by the Research Coordinator, a Statistician, and a Research Assistant. It provides support to all researchers in all the administrative and economical issues.
- Our current research areas which have been previously defined by the Research Committee are formed by a Coordinator and some members of the Institute (including residents and staff in training). The Research Committee also tries to distribute the staff in each area in a proportional way so each area has enough working in it.
- The organizational goals have been reviewed and approved by all staff
- A knowledge management sharing culture has been created
- Data is stored in a safer and more accessible way
- Being able to know the current status of our activities
- Propose corrective actions
- Learn from our mistakes and own experiences
- Transform individual knowledge into organizational knowledge
- Conduct deeper evaluations of our activities
- Transform information into knowledge
IS IT POSSIBLE TO IMPLEMENT A KNOWLEDGE MANAGEMENT SYSTEM IN A PUBLIC HOSPITAL ENVIRONMENT?
Berta Velasco1, José María Eiros2, Agustín Mayo3, Alberto San Roman1
1Institute of Heart Sciences (ICICOR), Cardiology Service, University Clinic Hospital.
2Microbiology Department, Faculty of Medicine, University of Valladolid.
3Statistics and Operations Research Department, Faculty of Medicine, University of Valladolid
Valladolid, Spain.
bvelasco @ icicor.es
Rev Electron Biomed / Electron J Biomed 2011;2:13-20
Comment of the reviewer José Luis Hernández Cáceres PhD. Profesor Titular de la Universidad Médica de La Habana. Cuba.
Comment of the reviewer María Jesús Coma MD. PhD. Research Unit. Complejo Asistencial Universitario de Burgos, España.
SUMMARY
This paper describes a conceptual organizing scheme for managing knowledge within a health setting. In this paper we present a framework to implement a Knowledge Management System (KMs) to manage and evaluate the research activities in a Cardiology Department of a Public Hospital in Spain. This framework was derived from a review and analysis of the knowledge management literature and from the author´s own experience.
KEY WORDS: Knowledge management. Knowledge translation. Health research. Information technology systems
RESUMEN:
Este artículo describe un plan conceptual para organizar la gestión del conocimiento en un entorno sanitario. Se presenta un marco para implementar un Sistema de Gestión del Conocimiento (KMs) para organizar y evaluar las actividades de investigación en un Servicio de Cardiología de un Hospital Público en España.
Este marco se ha desarrollado a través de una revisión y análisis de la literatura sobre la gestión del conocimiento y por las propias experiencias de los autores.
PALABRAS CLAVE: Gestión del conocimiento. Transferencia del conocimiento. Investigación sanitaria. Sistemas de tecnología informática
INTRODUCTION
The Institute of Heart Sciences (ICICOR) is formed by the Cardiology and Cardiac Surgery Departments of the University Clinical Hospital in Valladolid, Spain.
Our mission is to contribute to the improvement of the cardiovascular health within the population of Castile and Leon by promoting excellence in our activities: clinical assistance, teaching and research.
Our framework is focused just in our research activities because we understand health research as one of the elements of the welfare process since it is a strategy of intervention that instead of acting directly analyses and studies those health problems whose causes or solutions are still unknown. Health research also generates knowledge that has the potential to improve our citizens' health and strengthen healthcare systems and economies which should be a must in any public hospital, but unless this knowledge is put into action, these benefits will not be realized.
Before we explain our proposed knowledge management framework some basic notions of knowledge in our context must be reviewed for a better understanding of it.
Knowledge is something that comes from information processed by using data. It includes experience, values, insights, and contextual information and helps in evaluation and incorporation of new experiences and creation of new knowledge1. There are two types of knowledge: tacit and explicit knowledge. Tacit knowledge refers to a knowledge which is only known by an individual and that is difficult to communicate to the rest of an organization. On the other hand, knowledge that is easy to communicate is called explicit knowledge.
Knowledge management (KM) refers to the developing body of methods, tools, techniques and values through which organizations can acquire, develop, measure, distribute and provide a return on their intellectual assets2. KM is also an integrated, systematic approach to identify, manage, and share all of the organization's information assets, including databases, documents, policies and procedures, as well as previously unarticulated expertise and experience resident in individual officers3. KM creates a new working environment where knowledge and experience can easily be shared and also enables information and knowledge to emerge and flow to the right people at the right time so they can act more efficiently and effectively 4.
Knowledge Management Systems (KMs) are used to discover, develop, exploit, disseminate and share organizational knowledge5. Organizational knowledge has several dimensions: individual and group knowledge, internal and external knowledge, and tacit and explicit knowledge6.
Knowledge Management Framework (KMF) is very important for the organizations that intend to implement the KM system in their organization. It will become as the guidelines in order to avoid the errors and gain other benefits in terms of time and effort as well as cost involvement7.
In practice, the framework has to provide a coherent language and a point of view that enables the various organizational actors to see their activities within the overall effort to develop organizational knowledge management. This requires that the current state and the vision of the organization can be seen together, in a way that enables the organization developers to bridge the gap.
Knowledge translation (KT) is described a structured process that results in scientifically researched evidence being used to improve the outcomes of professional practice.
Although KT may relate to any science-based field, the term is most commonly associated with medicine and health care8.
The Balance ScoreCard (BSC) is a strategy-related performance measurement method which models an organization from innovation and learning, internal process, customer and financial perspectives. It provides a framework that not only provides performance measurements, but helps planners identify what should be done and measured. It also enables organizations to translate vision and strategy into action. KMs can assist organization in fulfilling innovation strategy. Thus, the integration of BSC and KMs derives from perspectives and KMs functions.
KMs need to be measured as any other management tool and need to be monitored as any other activity in any organization to trace its progress and result because just what can be measured can be managed. The success of KMs is not predictable and performance can be measured only after a long time period9.
A Strategy map is a diagram that is used to document the primary strategic goals being pursued by an organisation or management team. It is an element of the documentation associated with the Balanced Scorecard10.
Key Performance Indicators (KPI) are quantifiable measurements that reflect the critical success factors of an organization. Based on beforehand agreed measures, they reveal a high-level snapshot of the organization. They vary depending on the kind of organization they characterize; for instance a business may have a KPI as the annual sales volume, while KPIs of a health care facility may have to do more with patient satisfaction or the cost of the treatment11.
MATERIAL AND METHODS:
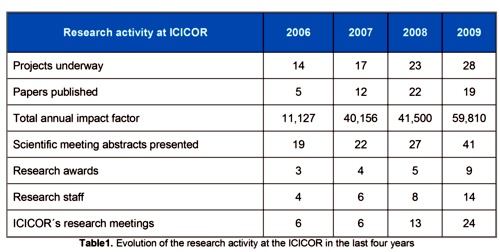
The evolution of our research activity in the last years (table 1) arose the idea of creating a KMs to manage this activity in a more effective way and also to create a knowledge culture within our institution.
This KMs will enable us to manage and evaluate our activities in different periods of time. We also want that the knowledge created by our research activity will be applied to the clinical practice in a faster way and that this knowledge could be used again in the future creating at the same time new knowledge. Our KMs will also allow that individual knowledge will be transformed into organizational knowledge.
In order to define our goals we have already designed a Balance Scorecard (BSC) following these steps (Figure 1):
1. We planned our strategy: we defined our mission, vision, and did a SWOT analysis (Strengths, Weaknesses, Opportunities, and Threats).
2. We created a strategic map: we defined our strategic objectives and their causality relations (Figure 2)
3. We identified our key performance indicators (KPI) and we also set the targets for each KPI
4. We developed our initiatives: we also identified our strategic actions to translate strategy into action.
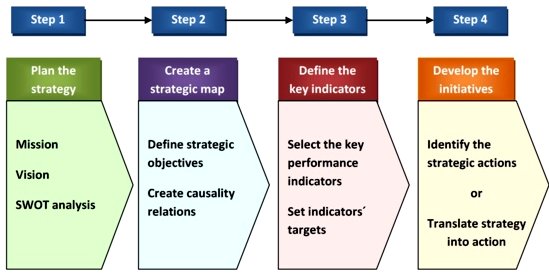
Figure 1. Steps to create a BSC at the ICICOR
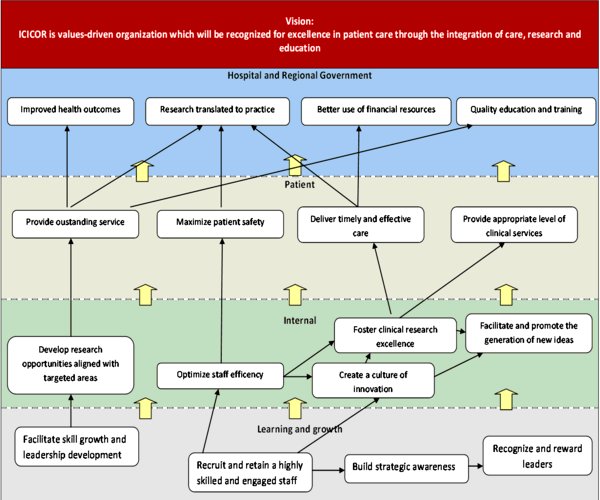
Figure 2. The strategic map at the ICICOR
All our key performance indicators have some common characteristics: they are objective, quantifiable, relevant, easy to understand, reliable, replicable, and delimited in time. And can be classified in three categories:
Indicators are independent since they measure different concepts and they cannot be reduced to a number. To know its evolution, indicators have to be compared in different periods of time.
The evaluation can carry out in different ways: overall to know the research activity of the institution, or by research groups to know the evolution of this specific research group, or individually to know the activity of each researcher.
In a health research context as ours, the knowledge life cycle can be represented as in Figure 3.
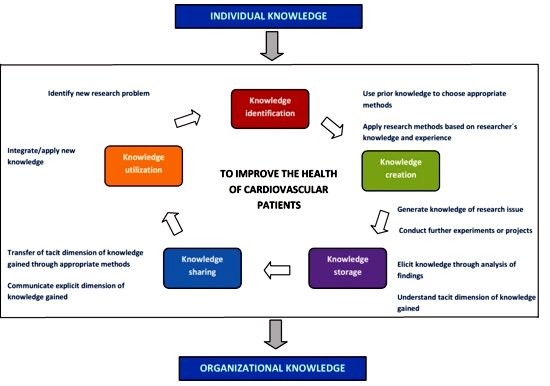
Figure 3. The knowledge life cycle at the ICICOR
Our proposal of knowledge management can be viewed as consisting of several dimensions where changed is needed and we have to address all of these to get knowledge management deployed.
-
1. The first dimension is conceptual, as we need to understand what knowledge is, how it is used, what does its management consists of, and how we could improve our knowledge processes to understand and manage knowledge in our organization in an efficient way. We have organized a set of informational meetings in order to inform our staff about these concepts.
2. The second dimension is change. Before new knowledge changes knowledge structures and systems of activity within our Service, knowledge has to be accessed, understood, and accepted. We have already designed a web based informatic tool to collect data, use and evaluate knowledge and also generate new knowledge which is structured in different modules:
Each module has an administrative interface for data entry and a user interface that enables browsing or searching of contents. Both are accessible through the Internet with security levels of controlling data access and manipulation, and a username and password are required to access the modules. We also believe that our tool will help us to understand better what our internal knowledge is. Our external knowledge comes from the periodical review of scientific papers, meetings with researchers from other institutions, congresses, experts' visits to our institution through our annual program "The experts in Valladolid" and also through our "short stays program" in which our researchers visit other institutions to learn new techniques for example.
3. The third dimension is measurement of knowledge. First of all, our Service has defined some goals focused in the research area and by measuring our knowledge we will be able to know if we are moving towards these goals or if not so we can implement corrective actions. The key performance indicators will allow evaluating our activities. Our system allows controlling the current evolution of all activities but the evaluation will be made annually. The implantation of this system has been done at the beginning of this year so at the moment we have not made any evaluation yet and we cannot say if the system is working properly or if we need to make some changes to it.
4. The fourth dimension is tools. Knowledge can be collected in different ways and we have already identified some of them and we should be able to identify more in the future (web-based informatic tool, web page, annual reports, leaflets, bulletins, work documents, meetings minutes etc )
5. The fifth and last dimension is formal and informal organizational structure. We will have to define new roles and responsibilities for effective knowledge management and discuss ways to implement formal, informal and communication structures that improve knowledge processing. To efficiently and effectively implement a KM Strategy and to perform the new KM processes, some new roles and responsibilities are required. These new roles and responsibilities may be absorbed within existing roles and/or they may be created as separate roles, depending on the scope, size and duration of the KM initiative. Some organizations have created dedicated roles, for example, a 'Chief Knowledge Officer' permanently, others have created the role for a few years until KM has become embedded throughout the organization, as part of its culture, and others have chosen not to introduce these new roles and responsibilities at all. The evidence shows that the most admired and successful KM initiatives have been those where these new focused roles and responsibilities are recognized and performed. In our institution, the roles have been created permanently to guarantee the success of the KM.
A 'knowledge worker' is not so much a new role, although it may be for certain organizations, but is considered to be recognition of a new responsibility for knowledge management and new personal knowledge management skills that all workers are expected to develop.
The organizational structure of the research area at the ICICOR has been decisive to define these new roles and responsibilities. This structure has been represented in Figure 4 and is composed by:
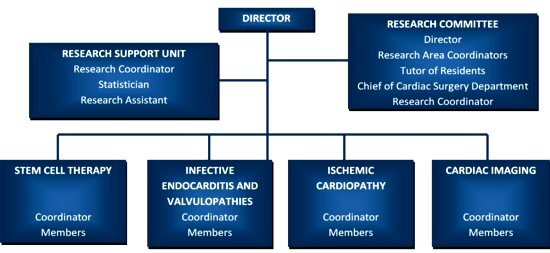
Figure 4. The organizational structure of the research area at the ICICOR
According to this organizational structure we have defined the new key roles and responsibilities as follows:
Chief Knowledge Officer: This role has been adopted by our Director. He is able to place KM within a theoretical and historical context as well as to critically appraise KM solutions and to manage organizational knowledge effectively, as a strategic asset, to further the organizations objectives.
Knowledge Manager: This role has been adopted by our Research Assistant. She is aware of the central importance and strategic benefits of KM and understands the underlying principles, processes, enabling tools and technologies. She is able to better manage knowledge effectively at an organizational and team level and she is also responsible for harvesting knowledge, ideas generated and to identify and critically assess the value of knowledge in the organization. She is aware of how the new communications, collaboration and information technologies effectively support the KM processes, within and between organizations. She is also able to audit existing KM processes and intellectual capital and to develop KM objectives and strategy to support inter-organizational and international organization KM processes as well as to educate and coach management and facilitate the change to a knowledge based organization. She keeps periodical meetings with the Director and with the Research Areas Coordinators in order to keep them informed about the development of these activities.
Knowledge Worker: This role has been adopted by our research line coordinators. He/she should be able to better manage knowledge effectively at an individual and team level and to manage information, time, tasks/processes and goals as well as to better access, filter, analyze, synthesize, accumulate, store, communicate and apply knowledge. He/she should also able to better collaborate in a dynamic, virtual team environment and to use communication, collaboration and information management technologies effectively to navigate the information and knowledge environment
RESULTS:
It is possible to implement a KMs in a Public Hospital environment. In our case, the KMs is focused in our research activities but it could had been also focused in our clinical activities for a better management of our clinical resources.
DISCUSSION:
A knowledge management system was implemented in our Department at the beginning of this year.
The system and its key performance indicators will be evaluated at the end of this year for the first time. This evaluation should provide us with the information necessary to decide if the proposed indicators to achieve our objectives should be modified or not.
Implantation of a knowledge management system should help us to translate the results of our research to the clinical practice in a faster way and also to manage our activities in a more effective way.
Success of KMs is not predictable and performance can be measured only after a long time period. Our KMs is quite young so we will need more time to evaluate its success but we believe that a knowledge sharing culture will only bring benefits not just for all researchers but for our institution in general. Some of the benefits of implementing a knowledge management system that we have already experienced are:
In our opinion, implementing a KMs is good for any organization as benefits can be achieved in a short period of time.
AKNOWLEDGEMENTS: This work was supported partially by the Spanish Cooperative Cardiovascular Disease Research Network (RECAVA, Red Temática de Investigación Cooperativa en Enfermedades Cardiovasculares) of the Spanish Institute of Health Carlos III from the Ministry of Science and Innovation.
REFERENCES:
-
1.- Abdullah R, Selamat M. A Framework for Knowledge Management System Implementation in Collaborative Environment for Higher Learning Institution. Journal of Knowledge Management Practice, 2005;6: March.
2.- Snowden D. Liberating knowledge. In: J. Reeves. Caspian Publishing (Editor), London. 1999. pp. 6-19
3.- Jones D. Knowledge and technical communication: a convergence of ideas and skills. 2003. Available at: https://faculty.washington.edu/markh/tc400
4.- Smith R. A roadmap for knowledge management. 2001. Available at: https://www2.gca.org/knowledgetechnologies/2001/proceeding
5.- Nissen ME. Knowledge-based knowledge management in the reengineering domain. Decision Support System. 1999;27:47-65
6.- Al-Ghassani AM, Robinson HS, Carrillo PM, Anumba CJ. A framework for selecting knowledge management tools, in Proceedings of the 3rd European Conference on Knowledge Management (ECKM 2002). Trinity College Dublin, 24-25 September 2002, pp. 37-48.
7.- Duffy J. The tools and technologies needed for knowledge management. Information Management Journal. 2001; 35: 64-67
8.- Landry R, Amara N, Pablos-Mendes A, Shademani R, Gold I. The knowledge-value chain: A conceptual framework for knowledge translation in health. Bulletin of the World Health Organization. 2006;84:597-602.
9.- Bontis N, Dragonetti NC, Jacobsen K, Roos, G. The knowledge toolbox: a review of the tools available to measure and manage intangible resources. European Management Journal 1999; August.
10.- Gupta S, Sharma SL, Dutta K. Using Knowledge mapping to support knowledge management in health organizations. Available at: https://library.igcar.gov.in/readit2007/conpro/s2/S2_5.pdf
11.- Bose R. Knowledge management metrics. Industrial Management & Data Systems. 2004;104(6):457-69.
CORRESPONDENCE:
Berta Velasco Gatón.
ICICOR. Hospital Clínico Universitario.
Avda Ramón y Cajal 3, Séptima Este.
47005 Valladolid. Spain
Mail: bvelasco @ icicor.es