Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
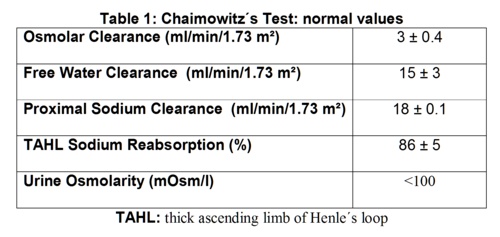
- Maximum urine hypotonicity (it reflects maximum urine dilution capability)
- Free water clearance (it reflects TAHL function)
- Proximal sodium clearance (it reflects proximal tubule function)
- TAHL sodium reabsorption (it reflects TAHL function)
- V = urine volume (ml/min)
- Osmolal clearance = urinary osmolarity x V / serum osmolaity (ml/min/1.73 m˛)
- Free water clearance = V - osmolal clearance (ml/min/1.73 m˛)
- Proximal sodium clearance = V x urinary sodium / serum sodium (ml/min/1.73 m˛)
- Potassium clearance = V x urinary potassium / serum potassium (ml/min/1.73 m˛)
- Sodium + potassium clearance = [(urinary sodium + urinary potassium) x V] / (serum sodium + potassium) (ml/min/1.73 m˛)
- Proximal tubule function = free water clearance + sodium clearance + potassium clearance (ml/min/1.73 m˛)
- TALH sodium reabsorption = free water clearance x 100 / free water clearance + sodium clearance (%)
COMPARISON BETWEEN TWO URINE DILUTION TESTS: THEIR ADVANTAGES AND DISADVANTAGES
Carlos G. Musso1, Matilde Navarro1, Hector Rivera1,
Guillermo Rosa Diez1, Juan F. Macías Núńez2
1Nephrology Division. Hospital Italiano de Buenos Aires. Buenos Aires. Argentina
2Nephrology Division. Hospital Universitario de Salamanca. Spain
carlosmusso @ gmail.com
Rev Electron Biomed / Electron J Biomed 2015;2:13-18.
Comment of the reviewer Amelia R. Bernasconi, MD. Head Department of Medicine. Hospital J.A. Fernández. Buenos Aires. Argentina.
Comment of the reviewer Dr. Ricardo Heguilen, MD. Nephrology Division. Hospital J.A. Fernández. Buenos Aires. Argentina
RESUMEN: COMPARACIÓN ENTRE DOS TEST DE DILUICION DE: SUS VENTAJAS Y DESVENTAJAS
La principal prueba fisiológica utilizada actualmente para la evaluación de la capacidad de dilución renal es la prueba de infusión hiposalina (PIH), la cual también evalúa la función del túbulo proximal y de la rama ascendente gruesa de Henle (RAGH).
Existe otra prueba de dilución de la orina: la prueba de sobrecarga acuosa oral, la cuál es más simple que la PIH. Sin embargo, no se ha documentado aun si la prueba de sobrecarga acuosa oral logra una evaluación adecuada del túbulo proximal y la actividad de la RAGH, como la PIH lo hace.
Por lo tanto, decidimos evaluar si había alguna diferencia significativa entre ambas pruebas mediante la evaluación de: la máxima capacidad de dilución urinaria, el aclaramiento proximal de sodio, y la reabsorción de sodio en la RAGH.
Materiales y Método: Ambas pruebas de dilución urinaria se realizaron de forma prospectiva a cuarenta voluntarios sanos con el objetivo de medir los siguientes parámetros fisiológicos: máxima hipotonicidad urinaria, aclaramiento de agua libre, reabsorción tubular proximal de sodio, y la reabsorción de sodio de la RAGH.
Resultados: Todos los voluntarios fueron capaces de diluir al máximo la orina durante PIH, mientras que sólo 4 voluntarios (10%) no fueron capaces de hacerlo durante las prueba de sobrecarga acuosa oral. No se hallaron diferencias significativa en los parámetros estudiados entre ambas pruebas, en aquellos pacientes que fueron capaces de diluir al máximo su orina (n: 36) (p = NS).
En conclusión, este estudio documentó que la prueba de infusión hiposalina y la prueba de sobrecarga acuosa oral, mostraron ambas ser estudios adecuados para evaluar la máxima capacidad de dilución urinaria, así como la funcionalidad tubular proximal y función de la RGAH. Sin embargo, mientras que la PIH fue más eficaz en la obtención de la dilución urinaria máxima, la prueba de sobrecarga acuosa oral, mostró ser un estudio más simple.
PALABRAS CLAVE: Fisiología renal. Dilución urinaria. Prueba fisiológica
SUMMARY:
The main physiological test currently used for evaluating renal dilution capability is the hypotonic infusion test (HIT), which also evaluates proximal and thick ascending limb of Henle´s loops (TALH) function.
There is another urine dilution test: oral water load test, and it is simpler than HIT. However, it has not been documented yet if oral water load test performs an adequate evaluation of proximal tubule and TAHL activity, as HIT does.
Thus, we decided to evaluate if there was any significant difference between both tests by evaluating: maximum urinary dilution capability, proximal sodium clearance, and TAHL sodium reabsorption.
Materials and Method: Both urine dilution evaluating tests were prospectively performed to forty healthy volunteers with the aim of measuring the following physiological parameters by them: maximum urine hypotonicity, free water clearance, proximal tubule sodium clearance, and TALH sodium reabsorption.
Results: All volunteers were able to maximally dilute their urine during HIT, while only 4 volunteers (10%) were not able to do it during the oral water load tests. No significant difference was documented in the three studied parameters between both tests, in those patients who were able to maximally dilute their urine (n: 36) (p= NS).
In conclusion this study has documented that HIT and oral water load test showed to be adequate studies for evaluating urine dilution capability, proximal and TAHL function. However, while HIT was more effective in obtaining the maximal dilution status, the oral water load test showed to be a simpler study.
KEY WORDS: Renal physiology. Urine dilution. Physiological test
INTRODUCTION
There are several clinical tests commonly used for evaluating different aspects of renal physiology1. The main physiological test currently used for evaluating renal dilution capability is the one called hypotonic infusion test or Chaimowitz´ test. This renal physiological test evaluates maximal urine dilution capability but also proximal tubule and thick ascending limb of Henle´s loops (TALH) sodium handling.
The Chaimowitz´ test is very reliable, safe and useful but it has the inconvenience of requiring the use of two intravenous lines and a continuous infusion pump2-3. On the other hand, there is another maximum urine dilution evaluating test, called oral water load test (OWLT), which is simpler than the Chaimowitz´ test. Since it is based on oral hydration it has the advantage of requiring only one intravenous line for blood sampling, and it has no need of continuous infusion pump. However, it has not been documented yet in the literature if OWLT performs an adequate evaluation of proximal tubule and TAHL sodium handling1.
Due to the above mentioned reason, we decided to evaluate if there was any significant difference between the Chaimowitz´ test and OWLT in evaluating maximum urinary dilution capability, proximal tubule, and TAHL sodium handling.
MATERIALS AND METHODS
Both maximum urine dilution evaluating tests, Chaimowitz and oral water load, were prospectively performed to forty healthy volunteers with the objective of obtaining the following physiological parameters from them:
For these purpose, the classical protocol described in the literature for performing both tests was followed1-2:
Chaimowitz ´ test2
The Chaimowitz' test, is based on the exploration of the tubular response to an acute fluid load. After fasting overnight, all participants received twenty cc/Kg of mineral water per os and two liters of intravenous hypotonic solution (0.66%) infused in two hours. Three blood samples were drawn (at 0, 60 and 120 minutes) and also urine samples were collected from each person at baseline (0 minute) and at 30 (±5) minutes intervals when voiding, and each urine volume was replaced by equal volume of mineral water per os (for keeping the urine rate) during the whole test.
From the obtained blood and urine samples glucose, urea, creatinine sodium, potassium, and osmolarity were measured, and then from the data corresponding to the most hypotonic urine sample (maximum dilution) and its corresponding blood sample three renal physiological parameters (proximal sodium clearance, free water clearance, sodium reabsorption TALH) were analyzed by applying the following formulas2-4:
Chaimowitz test normal result are shown in Table 1. Oral water load test1
After fasting overnight, volunteers received twenty cc/Kg of mineral water orally within 30 minutes. Three blood samples were drawn (at 0, 60 and 120 minutes) and also urine samples were collected from each person at baseline (0 minute) and at 30 (±5) minutes intervals when voiding, and each urine volume was replaced by equal volume of mineral water per os (for keeping the urine rate) during the whole test. From the obtained blood and urine samples glucose, urea, creatinine, sodium, potassium, and osmolarity were measured. A normal result is obtained when the subjects urinate more than 80% of the water load over 4 hours, and produce urine with an osmolarity of less than 100 mOsm/l following the test1.
Even though, in the classical version of this test, which is based on the same physiological principles than the Chaimowitz ' test, only maximun urine hypotonicity is documented, in this study proximal sodium clearance, free water clearance, and TALH sodium reabsorption were also documented from the most hypotonic urine sample (maximum dilution). All these parameters were obtained by applying the same formulas used in the Chaimowitz ' test in order to be able to compare both findings.
This study was approved by the Institutional Review Board and all participants provided written informed consent prior to the performance of the physiological tests.
Comparisons between both tests was performed with Student t test, with p<0.05 as the level of significance
RESULTS
All volunteers (n: 40) were able to maximally dilute their urine during the hyposaline infusion test (Chaimowitz' test), while only 4 volunteers (10%) were not able to do it during the OWLT. (Table 1)
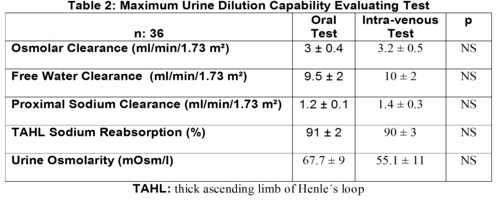
No significant difference was documented in the studied parameters: maximun urine hypotonicity, free water clearance, proximal tubule sodium clearance, and TAHL sodium reabsorption, between both test in those patients who were able to maximally dilute their urine (n: 36) (p= NS) (Table 2).
DISCUSSION
It is classically stated that the salt and water load infused during Chaimowitz' test suppresses the activity of anti-diuretic hormone (ADH) and aldosterone and thus "defunctionalizes" the collecting tubules. Sodium is the major solute reabsorbed at the proximal tubule, and thus the function of this segment can be analyzed through its local sodium clearance.
In contrast, water handling may account for the evaluation of the TALH, since this segment is responsible for the generation of free water clearance (or local sodium reabsorption) which, in turn, contributes to medullar hypertonicity and consequently to the water reabsorption capability in the collecting tubules under water restriction. Due to the afore mentioned reason, the Chaimowitz' test is able to evaluate proximal sodium function by measuring its sodium clearance, and TALH function by measuring free water clearance and its sodium reabsorption4-5.
In the present study, it was evaluated if oral water load was also an adequate test for documenting proximal sodium and TALH functions. It was found that, despite 4 volunteers not being able to maximally dilute their urine during OWLT, most of them were able to do so, and their measured physiological parameters were in normal range (Table 1) and their values showed no significant difference between the two tests (Table 2).
Regarding why few patients were not able to maximally dilute their urine only during the OWLT, this phenomenon could be attributed to the way of hydration (non-intravenous), and its lower amount (volume/minute) of water load used by this test.
Based on the above mentioned findings, and since OWLT is the easier test of the urine dilution evaluating tests, it could be suggested that the OWLT could be initially used in order to evaluate urine dilution capability, proximal tubule and TAHL function, and if the patient would not be able to adequately reduced his/her urine osmolarity: it means a urine osmolarity higher than 100 mOsm/l, the Chaimowitz' test should be performed in order to reconfirm this urine dilution defect.
In conclusion this study has documented that the Chaimowitz ' test and oral water load test showed to be adequate studies for evaluating maximum urine dilution capability, proximal and TAHL functions. However, while the Chaimowitz' test was more effective in obtaining the maximal dilution status, the oral water load test showed to be a simplest test to perform.
REFERENCES
1.- Berl T, Henrich W. Disorders of hydration. In Duarte C (Ed.) Renal function tests. Boston. Little, Brown and Company: 101-118
2.- Chaimovitz C, Levi J, Better OS, Oslander L, Benderli A. Studies on the site of renal salt loss in a patient with Bartter's syndrome. Pediatr Res. 1973;7(2):89-94.
3.- Macías Núńez JF, García Iglesias C, Bondía Román A, Rodríguez Commes JL, Corbacho Becerra L, Tabernero Romo JM, De Castro del Pozo S. Age Ageing. 1978;7(3):178-81Renal handling of sodium in old people: a functional study.
4.- Musso C, Fainstein I, Kaplan R, Macías Núńez JF. [Renal tubular function in the oldest old]. Rev Esp Geriatr Gerontol 2004; 39(5): 314-319
5.- Musso CG, Macías-Núńez JF. Dysfunction of the thick loop of Henle and senescence: from molecular biology to clinical geriatrics. Int Urol Nephrol. 2011;43(1):249-52
CORRESPONDENCE:
Dr. Carlos Musso
Departamento de Nefrología y medio Iterno.
Hospital Italiano de Buenos Aires.
Buenos Aires. Argentina
Mail: carlosmusso @ gmail.com
Comment of the reviewer Amelia R. Bernasconi, MD.
Head Department of Medicine. Hospital J.A. Fernández, Buenos Aires, Argentina.
Tests to assess renal function are usually tedious for both patients and operators.
The authors, who are usually dedicated to facilitate and simplify the diagnostic process of physiological tests, performed in this work an interesting comparison of the methods currently available for evaluating renal tubular maximum dilution.
Chaimowitz test requires the administration of parenteral solutions to explore both the renal tubular response to an acute overload, and the behavior of different nephron segments responsible for its control. The oral water load test prevents parenteral fluid, simplifying this procedure.
The successful review of the literature conducted by Dr. Musso and his collaborators, is easy to read and understand, allowing an update on our knowledge on this topic and the possibility of faster diagnosis.
Comment of the reviewer Dr. Ricardo Heguilen MD. Nephrology Division. Hospital J.A. Fernández. Buenos Aires. Argentina
Kidney function tests or better called dynamic renal functional tests are vital for evaluating this organ physiology and also for elucidating the pathophysiological mechanisms on which are based many renal conditions.
Fundamental premises for the applicability of these tests are basically their simplicity, reproducibility and especially safety for the individual subjected to them.
In this article the authors compared two methods to assess proximal tubule and loop of Henle function, as well as the maximum urinary dilution capability. Clearly demonstrated here, the consistency of results between both approaches showed that the oral water load test would be a simpler and less invasive test with similar cost / effectiveness.