Indice del volumen Volume index
Comité Editorial Editorial Board
Comité Científico Scientific Committee
UNCOMPLICATED CYSTITIS TREATED WITH HIGH PROANTHOCYANIDINS CRANBERRY CONCENTRATION IN PATIENTS AGED 70 YEARS OLD AND BELOW WITH RECURRENT URINARY TRACT INFECTIONS
Jesús J Cuadrado-Blanco MD.1 Guzman Tamame Gonzalez MD., PhD.2,3, Agapito Gomez Villa MD.4, Amparo del Cańizo MD.5, Juan F. Macías Núńez MD., PhD.6
1Medical Director and Urinary Incontinence Department Director. Salamanca. 2Residencia de Personas Mayores "Los Tres Árboles" de la Junta de Castilla y León; 3Centro de Día "Ciudad Jardín" de la Asociación de Familiares de Alzheimer, Zamora. 4Centro de Salud "Zona Centro", Cáceres; 5Centro de Salud Sancti Spiritus-Canalejas; 6Director FIIPERVA chair. University Salamanca, Salamanca. Spain
Email: jfmacias @ usal.es
Rev Electron Biomed / Electron J Biomed 2018;2:9-16.
Comment of the reviewer José R Jauregui MD, PhD Geriatrician. Hogar Ledor Vador. Buenos Aires, Argentina.
Comment of the reviewer Laura C Pezzano Pegorer, MD. Internal Medicine physician. Hospital Italiano de Buenos Aires, Argentina.
RESUMEN: CISTITIS NO COMPLICADA TRATADA CON ALTA CONCENTRACIÓN DE PROANTOCIANIDINAS DE ARÁNDANO EN PACIENTES DE 70 AŃOS O MENOS CON INFECCIONES RECURRENTES DEL TRACTO URINARIO
El objetivo de nuestro estudio fue evaluar originalmente la eficacia y seguridad de Cysticlean® (CYS), un extracto de cramberry que contiene 240 mg de proantocianidinas (PAC) por píldora, para tratar y prevenir la infección urinaria recurrente (rUTI) en pacientes adultos menores de 70 ańos y evaluar si: un ańo de tratamiento con CYS podría modificar o no varios parámetros de la función renal, así como la evaluación funcional geriátrica en aquellos pacientes entre 60 y 70 ańos.
Material y métodos: Se estudiaron 27 pacientes, con edades entre 53-70 ańos. En todos ellos se evaluó el antecedente rUTI confirmando al menos 3 episodios de infección urinaria / ańo. Todos los pacientes incluidos recibieron instrucciones de suspender los antibióticos durante un período de lavado de dos semanas antes de introducir CYS en un régimen de 1 cápsula de CYS por la mańana y 1 cápsula por la noche hasta que se controlaron los signos y síntomas de la cistitis. Los pacientes que sufrieron un nuevo episodio de infección urinaria durante el período de tratamiento con CYS lo detuvieron y fueron tratados de acuerdo con el mejor antibiótico necesario. Estos pacientes fueron considerados como un fracaso del tratamiento con CYS.
Resultados: Veintiún pacientes no sufrieron infección urinaria durante el período de estudio. Entre ellos, 17 eran mujeres y 4 hombres (p <0,044). Solo 6 pacientes (2 mujeres y 4 hombres) sufrieron una infección urinaria en el período de estudio. Todos estos tratamientos fallidos de CYS fueron tratados con antibióticos apropiados. CYS no modificó la función renal de los pacientes ni el estado funcional de los pacientes en este estudio.
Conclusión: Cysticlean® es un extracto de arándano americano que ha podido controlar la rITU en el 78% de los pacientes tratados en este estudio gracias a su alta actividad antiadhesiva proporcionada por su muy alta concentración de PAC. No se informaron efectos secundarios ni reacciones adversas.
PALABRAS CLAVE: Arándano, vaccinium macrocarpon, Cysticlean®, proantocianidinas, cistitis, infecciones del tracto urinario.
ABSTRACT:
The objective of our study was to originally evaluate the efficacy and safety of Cysticlean® (CYS), a cramberry extract which contains 240 mg of proanthocyanidins per pill, to treat and prevent recurrent urinary tract infection (rUTI) in adult patients younger than 70 years old and to evaluate if one year of treatment with CYS could modify or not several parameters of the renal function, as well as the geriatric functional evaluation in those patients between 60 and 70 years old.
Material and methods: 27 patients were studied, aged 53-70 years. In all of them was evaluated rUTI antecedent confirming at least 3 episodes of UTI/year. All included patients were instructed to stop antibiotics for a washing out period of two weeks before introduce CYS in a regime of 1 capsule of CYS in the morning and 1 capsule in the evening up to the signs and symptoms of cystitis were controlled. Patients who suffered from a new episode of UC during the CYS treatment period stopped it and were treated accordingly to the best antibiotic needed. These patients were considered as a fail of the CYS treatment.
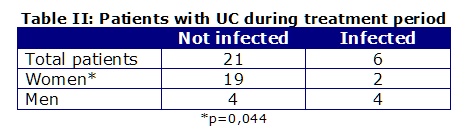
Results: Twenty-one patients did not suffer any UC during the study period. Among them 17 were women and 4 men (p<0,044). Only 6 patients (2 women and 4 men) suffered a UC in the study period (Table II). All this failed CYS treatments were treated with appropriate antibiotics. CYS modified neither patients´ renal function nor patient´s functional status in this study.
Conclusion: Cysticlean® is an American cranberry extract who has been able to control the UTI in 78% of patients treated in this study thanks to its high anti-adhesion activity provided by its very high PAC concentration. Neither side effects nor adverse reactions were reported.
KEY WORDS: Cranberry, Vaccinium macrocarpon, Cysticlean®, Proanthocyanidins, cystitis, Urinary tract infections, UTIs.
INTRODUCTION
Recurrent urinary tract infection (rUTI) is a very frequent disease in children with congenital urological diseases, fertile ladies and old women and men worldwide1.
These infections are usually defined as uncomplicated cystitis (UC) when fever and general discomfort are not present. Up to 75% of all UC are caused by Escherichia coli (Ec), and no differences have been found among countries regarding its prevalence. Ec is a saprophyte bacterium in the human gut, which becomes a pathological one in the human urinary tract1,2.
Symptoms and signs of UC included local ones like abdominal pain, dysuria, pollakiuria, emergency to urination and itching among others. Leucocyturia and hematuria (macro and micro) are also frequent and the urine culture is usually positive, mainly to Ec. There are patients, mostly old patients that show positive urine culture without symptoms and signs of UC. In fact, it is difficult to consider this positive urine culture as a sign of UTI/UC unless the total number of colonies of bacteria is higher than 100.000/field2.
UC is usually successfully treated with antibiotics. However, the bacterial antibiotic resistance is an important current problem which leads to look for alternative therapeutic strategies. Bacteria antibiotic resistance is not an exclusive problem of UC treatment, but it has been described as a global problem, and being currently considered one of the most important health issue world-wide3,4.
Since late sixties in the XX century, non-antibiotic products have been used as an alternative to mainly prevent rUTI. Among them the most common ones have been vitamin C, D-mannose and cranberry extracts. It was considered that vitamin C could reduce the urinary pH to reduce the infectious capacity of several bacteria. However, the doses of vitamin C needed to reduce the urinary pH were very high (4 g/day), therefore it use was discontinued. In this sense, the D-mannose was also used with controversial results. However, now a day these products start to be used due to the documented currently bacteria antibiotic resistance5,6.
Regarding the American cranberry fruits, they were used with medical purpose by Canadian First Nations during the XIX century, then its use was abandoned when the antibiotics era started, but they have come back late in the XX century. Cranberry extracts have proven to be quite effective to treat and prevent rUTI due to its anti-adhesion effect against Ec thanks to the proanthocyanidins (PAC) concentration (7-13). More recently, several studies have proven a strong relationship between PAC concentration and anti-adhesion activity. Unfortunately, the lack of a standard analysis method to evaluate PAC concentration of cranberry extracts, as well the lack of information about the anti-adhesion property of many of the cranberry extracts available, are not facilitating its standards use as the first step to treat and prevent UC and rUTI caused by Ec. Cranberry extracts were originally suggested to be used to prevent Ec urinary re-infections by Cochrane Institute in 2008 and the European Urologist Association, however these recommendations were not maintained due to lack of clinical studies, lack of a standard PAC analysis method, and lack of information of its anti-adhesion property14-21.
Cysticlean®(CYS) is a very high PAC (240 mg capsule/sachet) concentrated cranberry extract that shows a high anti-adhesion activity against Ec (up to 80%) which is related to PAC concentration22. Several published studies have documented its safety and efficacy profile to for treating and preventing rUTI and UC. More than 600 patients in different studies have been treated with CYS showing an effective prevention of rUTI in different populations: children with congenital urological disease, fertile and postmenopausal women, post-coital infections and elderly people, successfully treated up to 1 year or more. No side effects /adverse reactions have been reported associated to this product22-23.
The objective of our study was to originally evaluate the efficacy and safety of CYS to treat and prevent rUTI in adult patients younger than 70 years old and to evaluate if one year of treatment with CYS could modify or not several parameters of the renal function, as well as the geriatric functional evaluation in those patients between 60 and 70 years old.
MATERIAL AND METHODS
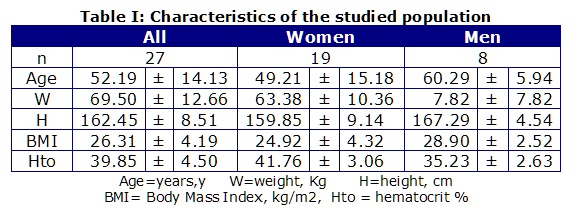
In this study 27 patients were included: 8 men aged 53-70 years (x: 61.5 ± 6.5) and 19 women aged 18-68 years old (x: 49.2 ± 15.2). In all of them was evaluated rUTI antecedent confirming at least 3 episodes of UTI/year (Table I).
Exclusion criteria were: patients younger than 18 years or older than 70 years, presence of pregnancy, or active oncologic disease.
Inclusion criteria were: patients who were complaining from a new episode of symptomatic cystitis.
Basic demographic data and renal functional parameters were obtained from all patients. Furthermore, patients aged between 60 and 70 years were completely assessed for physical, psychological, functional and social status (quadruple geriatric evaluation) before and after proanthocyanidins cranberry extract treatment.
All included patients were instructed to stop antibiotics for a washing out period of two weeks before introduce CYS in a regime of 1 capsule of CYS (240 mg of proanthocyanidins cranberry extract) in the morning and 1 capsule in the evening up to the signs and symptoms of cystitis were controlled. Patients who suffered from a new episode of UC during the CYS treatment period stopped it and were treated accordingly to the best antibiotic needed. These patients were considered as a fail of the CYS treatment.
Written informed consent was obtained from all patients involved in the study. This study was carried out in accordance with the Helsinki Declaration (2000) of the World Medical Association and was performed in accordance with the principles of Good Clinical Practice.
Statistical analyses were performed using PASW Statistic 18 (SPSS) (2009, IBM Company, Chicago, Illinois). Standard descriptive statistics were used (mean ± standard deviation, max, min, and n) for continuous measurements. univariate correlations (Pearson coefficient) between patient's characteristics (ages, sex and weight), number of signs and were calculated using a two-sided p-value. Comparative evaluation (t test) were performed for comparison; p-value of <0.05 was considered statistically significant.
RESULTS
In this study female patients were less weighted, smaller, younger and had a lower body mass index and slightly lower hematocrit compared to male patients. The glomerular filtration rate (GFR) according to the age ranged 65,6 -105,6 ml/min (women: 65.6 -105.6 ml/min, men: 74.0 - 87.6 ml/min), estimated GFR (by Gregori-Macías equation) ranged 38.0 - 142,98 ml/min (women: 47.56 - 142.9 ml/min, men: 38 - 78.9), serum creatinine (Cr) ranged 0.47 - 2.54 mg/dl (women: 0.47 - 1.98, men: 0.83 -2.54), serum urea (U) ranged 15.0 -75 mg/dl (women: 15.0 - 72 mg/dl, men: 29 -75 mg/dl), chronic kidney disease screening equation (HUGE equation) ranged +5.08 to -7.38 (women: -7.38 to -0.07, men: -3.69 to +5.08). Geriatric assessment remained unchanged along the CYS treatment.
Twenty-one patients did not suffer any UC during the study period. Among them 17 were women and 4 men (p<0,044). Only 6 patients (2 women and 4 men) suffered a UC in the study period (Table II). All this failed CYS treatments were treated with appropriate antibiotics.
No side effects/adverse reactions were reported during the study. The elapsed time between the start of the treatment and clear up of clinical and bacteriological episode ranged between 3.3-14.8 months (x: 5.3±2.4 months).
At the end of the study, evaluated renal functional parameters showed that women had a significantly lower serum creatinine, serum urea and HUGE values, as well as higher GFR values than men (Table III).
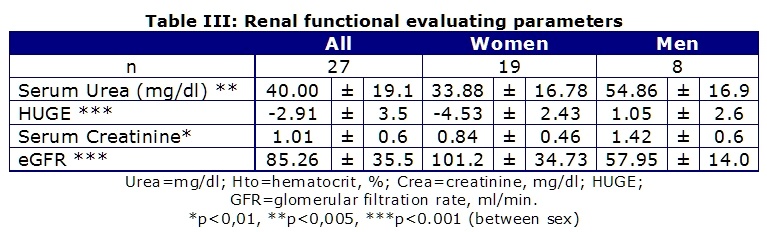
Due to the size of the sample of this study it is difficult to get any conclusion from these data, but it could suggest that UTI may be more frequent in men with slightly reduction of their renal function (Table III).
Further studies on this area should be performed to better know if impaired renal function could be a risk factor of recurrent UTI.
No patient reported any side effect/adverse reaction related to CYS treatment during the study, and cystitis was well controlled in all patients with CYS or antibiotics depending on UC responded to CYS or fail to respond to it, respectively.
DISCUSSION
UTI treatment is on focus of all infections due to their high incidence (2nd infection in the world), being up to 80% caused by E. coli, and the non-stop increasing bacteria antibiotic resistance1,2.
According to the UTI characteristics, it seems that alternative non-antibiotic treatments are crucial to be evaluated due to the increasing frequency of antibiotic. From XIX century American cranberry extracts have been used to treat UTI. Unfortunately, lack of cranberry extracts standardization, the influence of the antibiotic era and a non-scientific approach on the use of vitamin C to treat UTI, has made difficult the recognition of its utility3-5.
Since late XX and further, antibiotic resistance has increased again the interest on American cranberry extracts to prevent and treat UTI7.
It is worth pointing out that 2008 Cochrane review recommended the use of such extracts to prevent UTI. Unfortunately, almost all American cranberry products in Europe are commercialized as food supplements. Until August 2017, there were very little sold as a medical product due to its anti-adhesion effect was not considered a pharmacologic action. However, the European Community commission decides that such effect was not a pharmacologic action and then these products were not allowed to continue to be commercialized as medical product. Many studies published since 2004 and beyond have proven that E. Coli adhesion to the inner wall of urinary bladder was directly related to the PAC concentration and such effect was directly related to its efficacy to prevent and treat UTI15-20.
In addition, there is currently a real problem to use these extracts as an alternative to antibiotics to treat and prevent UTI because, as food supplements, is not possible to write any medical claim on their labels. Furthermore, there are not clinical trials performed with American cranberry extracts as food supplements and there are not any standard criteria to fix the PAC concentration and the anti-ad hesi ctivity of these products to be used as an alternative to antibiotics. This one of the biggest health problem facing by the world and not too many alternatives are available to antibiotics to treat Ec UTI apart from the documented American cranberry extract products.
CYS with a very high anti-adhesion activity, secondary to its very high PAC concentration, has proven its safety and efficacy to treat and prevent UTI in children, elderly, post coital, fertile and postmenopausal women with no side effects/adverse reactions reported since first commercialization in 2007 22-23.
In this study, it was confirmed the high proportion of patients who did not need any antibiotic to treat and prevent their UTI. Furthermore, it was documented that CYS modified neither the renal functional parameters nor the functional status in the studied patients aged 60-70 years.
CONCLUSSION
Cysticlean® is an American cranberry extract who has been able to control the UTI in 78% of patients treated in this study thanks to its high anti-adhesion activity provided by its very high PAC concentration. Neither side effects nor adverse reactions were reported. Furthermore, Cysticlean® modified neither patients´ renal function nor patient´s functional status in this study.
REFERENCES
1. Tandogdu Z, Wagenlehner F. Global epidemiology of urinary tract infections,?Current Opinion in Infectious Diseases.2016;29(1):73-79.
2. Flores-Mireles A, Walker J, Caparon M, Hultgren S. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol 2015; 13(5): 269-284.
3. Lee C, Ventola P. The Antibiotic Resistance Crisis. Part 1: Causes and Threats.2015;40(4): 277-283
4 . Blair J, Webber M, Baylay A, Ogbolu D, Piddock L. Molecular mechanisms of antibiotic resistance. Nature Reviews Microbiology. 2015;13: 42-51.
5 . Van Puyvelde S, Deborggraeve S, Jacobs J. Why the antibiotic resistance crisis requires a One Health Approach.The Lancet. 2018;18(2):132-134
6. Garat Barredo JM. Treatment of paediatric urinary infections with American cranberry extract. Acta Pediátrica Espańola. 2011; 69(3): 117-120.
7.- Beerepoot M, Geerlings S. Non-Antibiotic Prophylaxis for Urinary Tract Infections. Pathogens 2016;5:36
8.- Beerepoot M, Riet G, Nys S, van der Wal W, de Borgie C, de Reijke T, Prins J, Koeijers J, Verbon A, Stobberingh E, Geerlings S. Cranberries vs Antibiotics to Prevent Urinary Tract Infections: A Randomized Double-blind Noninferiority Trial in Premenopausal Women. Arch. Intern. Med. 2011;171: 14-25
9.- Finkelstein R, Kassis E, Reinhertz G, Gorenstein S, Herman P .Community-acquired urinary tract infection in adults: a hospital viewpoint.. J Hosp Infect. 1998 Mar;38(3):193-202.
10.- McMurdo ME, Argo I, Phillips G, Daly F, Davey P. Cranberry or trimethoprim for the prevention of recurrent urinary tract infections? A randomized controlled trial in older women. J Antimicrob Chemother. 2009;63(2):389-95.
11.- Uberos J, Nogueras-Ocana M, Fernández-Puentes V, Rodríguez-Belmonte R, Narbona-López E, Molina-Carballo A, Muńoz-Hoyos A. Cranberry syrup vs trimethoprim in the prophylaxis of recurrent urinary tract infections among children: a controlled trial. Open Access Journal of Clinical Trials.2012:4 31-38
12.- Caljouw M, van den Hout W, Putter H, Achterberg W, Cools H, Gussekloo J. Effectiveness of Cranberry Capsules to Prevent Urinary Tract Infections in Vulnerable Older Persons: A Double-Blind Randomized Placebo-Controlled Trial in Long-Term Care Facilities.. JAGS.2014; 62:103-110
13. Vostálová J, Vidlar A, Simánek V, Student V. Are High Proanthocyanidins Key to Cranberry Efficacy in the Prevention of Recurrent Urinary Tract Infections?. Phytotherapy Research. 2015;29: 10
14 - Mayor S. Cranberry capsules do not reduce urinary tract infections in older women, study finds. BMJ 2016; 355 doi: https://doi.org/10.1136/bmj.i5835
15.- Singh I, Gautam L, Kaur IR. Effect of oral cranberry extract (standardized proanthocyanidin-A) in patients with recurrent UTI by pathogenic E. coli: a randomized placebo-controlled clinical research study. Int Urol Nephrol. 2016;48(9):1379-1386.
16.- Howell A, Botto H, Combescure C, Blanc-Potard A, Gausa L, Matsumoto T, Tenke P, Sotto A, Lavigne J.Dosage effect on uropathogenic Escherichia coli anti-adhesion activity in urine following consumption of cranberry powder standardized for proanthocyanidin content: a multicentric randomized double blind study. BMC Infect Dis. 2010; 10: 94. 10.1186/1471-2334-10-94.
17.-Risco-Rodríguez E, Álvarez-Sala W, Ramos VC, Bonet I. Concentration-Dependent Effect On Adherence Of Escherichia Coli To Bladder Epithelial Cells Of Cysticlean Capsules (240 Mg/Capsule Of Proanthocyanidins). The Internet Journal of Microbiology;13(1).
18.- Howell AB, Botto H, Combescure C. Dosage effect on uropathogenic Escherichia coli anti-adhesion activity in urine following consumption of cranberry powder standardized for proanthocyanidin content: a multicentric randomized double blind study. BMC Infect Dis 10: 94.
19.- Garat J.M. Treatment/prevention of urinary infections in children using cranberries. Urol Integr Invest 2009:14(2).
20.- Bonet I, Batista E, Conejero J, Cortadellas L, Mandańa A, Peyrí E, Pigrau A, Urmeneta JM. Vargas C, Viladoms JM. Cranberries in the treatment of cystitis. Urol Integr Invest 2008;13(3):214-217.
21.- Collado A, Trassierra M, Monllor E, Navalón R, Tramoyeres A, Ordońo F, Osca J, Gómez A, Monzonís L, Dumont R.Observational study of using American cranberry extract rich in proanthocyanidins to treat recurrent urinary tract infections. Urol Integr Invest 2009;14(4):366-369.
22.- Sánchez-Ballester F, Ruiz-Vidal V, López-Alcina E, Doménech-Perez C, Escudero-Fontano E, Oltra-Benavent A, Montoliu-García A, Sobrón-Bustamante M. Cysticlean® a highly PAC standardized content in the prevention of recurrent urinary tract infections: an observational, prospective cohort study.BMC Urology 2013, 13; 28
23.- Risco-Rodríguez E, Suárez H, Bonet I, Cuadrado-Blanco J. Evaluation Of Cysticlean® Capsules, A Cranberry Extract With High Anti-Adhesion Activity, As Monotherapy In Uncomplicated Cystitis: An Observational Pilot Study. Rev Electron Biomed / Electron J Biomed 2015;2:19-28.
CORRESPONDENCE:
Dr Juan F. Macías-Núńez
Director FIIPERVA
Universidad de Salamanca
Salamanca.Espańa
Email: jfmacias @ usal.es
Comment of the reviewer José R Jauregui MD, PhD. Geriatrician. Hogar Ledor Vador. Buenos Aires, Argentina.
The objective of the study was to originally evaluate the efficacy and safety of CYS to treat and prevent rUTI in adult patients younger than 70 years old and to evaluate if one year of treatment with CYS could modify or not several parameters of the renal function, as well as the geriatric functional evaluation in those patients between 60 and 70 years old, and this objective was obtained.
Comment of the reviewer Laura C Pezzano Pegorer, MD. Internal Medicine physician. Hospital Italiano de Buenos Aires, Argentina.
This study tries to prove an alternative treatment to antibiotics for urinary infection (UI), and the extract of cranberry for its effect of avoiding the adhesiveness of E. Coli can be a valid alternative. Anyway, the number of patients in the study does not allow us to draw valid conclusions and more research is necessary to determine it.
Furthermore, it was documented that CYS modified neither the renal functional parameters nor the functional status in the studied patients aged 60-70 years.
Further studies on this area should be performed to better know if impaired renal function could be a risk factor of recurrent UI.